- Visibility 56 Views
- Downloads 15 Downloads
- DOI 10.18231/j.idjsr.2024.022
-
CrossMark

Vertical dysplasia
- Author Details:
-
 Kuchana Aparna *
Kuchana Aparna *
-
Seena Naik
-
M Thirumal Naik
-
Rahul Goud Padala
-
Sumedha Surendranath Malshetwar
-
Vyshali Kothamasu
Introduction
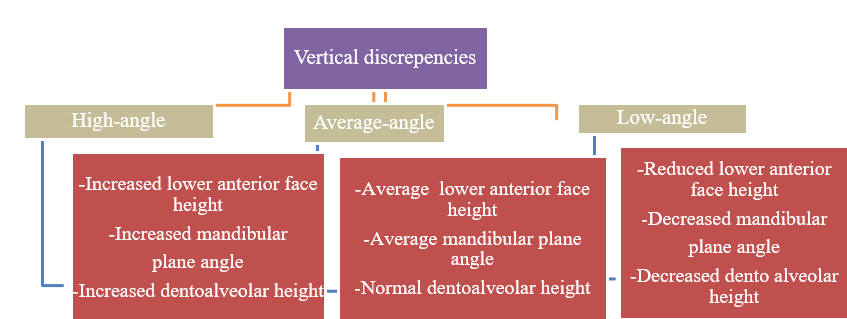
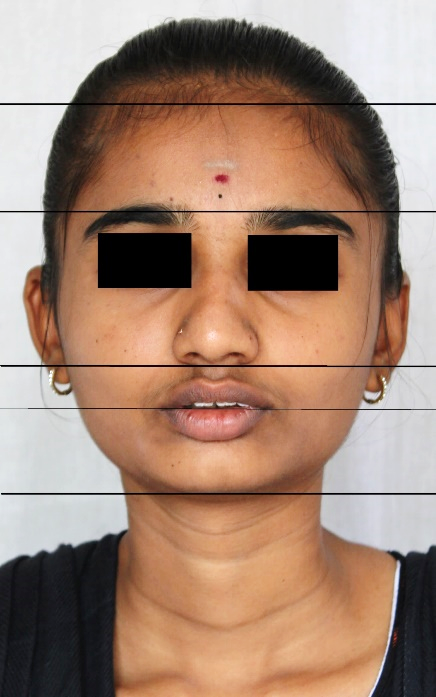
The vertical dimension of the lower face is a prerequisite for facial balance harmony. Vertical dimension is the relationship between the Frankfort and mandibular planes or it may also be defined as the relative relationship between the anterior and posterior facial heights.[1] Its importance was first recognized by Downs and later by Wylie and Johnson.[2] Frakas and Frakas and Munro[3] divided the face vertically into equal thirds horizontal lines at the hairline, bridge, and ala of the nose and menton, and the lower third of the face was further divided into the upper third and lower two thirds ([Figure 3]). Assessment of the vertical proportions helps in the better diagnosis of problems in the vertical dimension of the face. Increased lower facial height may be due to either vertical maxillary excess or excessive height of the chin.[3] The following are the most commonly used different terms to describe the condition. They are dolichofacial, leptoprosopic, hyperdivergent, skeletal open bite, high angle, backward rotator, adenoid faces, long face syndrome, and vertical maxillary excess ([Figure 4]).[2] Decreased lower facial height may occur due to either vertical maxillary deficiency or decreased chin height.[3] Different terms are used to describe the condition as brachycephalic, euryprosopic, hypodivergent, skeletal deep bite, low angle, forward rotator, short face syndrome, and vertical maxillary deficiency ([Figure 5]).
According to Haas,[4] patients with vertical discrepancy exhibits the following features:
Poor facial depth
Short posterior facial height, viz., a short mandibular ramus and antegonial notching in mandible
Body with deficient height at molar area and excessive height at the symphysis
Poor depth to the symphysis compared with the height
Lack of chin button
An anterior slope to the anterior surface of the symphysis
Classification of vertical discrepencies
Skeletal classification of basic facial types
According to Sassouni,[5] there are two basic types with vertical disproportions (the skeletal deep-bite and open-bite).
According to Ashok karad,[6] vertical discrepancies are divided into the following categories:
Dental
According to Graber,[7] vertical relationships are divided into four major categories:
Anterior open bite
Anterior deep bite
Posterior open bite
Posterior collapsed bite with overclosure
Open bite and deep bite exhibit variation in both skeletal and also in dental types ([Table 1]).
Development of Vertical Discrepencies
During the growth period because of the interplay of many etiological factors, vertical malocclusions may develop.[8] Vertical malocclusions can be divided into those that are dentoalveolar in origin and those that are predominantly skeletal due to the growth patterns of the jaw.[8] Facial growth with the cranial base proceeds along a vector with variable amounts of horizontal and vertical growth. It is important to understand and appreciate the value of vertical growth, as it relates to anteroposterior growth. Vertical growth carries the chin downward, while anteroposterior growth carries it forward. The major sites of bony additions contributing to facial growth include the facial sutures, maxillary alveolar processes, mandibular condyle, and mandibular alveolar processes.[9] If vertical growth increments at the facial sutures and the maxillary and mandibular alveolar processes exceed the condylar growth, the mandible will rotate backward. However, if growth at the condyle exceeds the total vertical growth at the facial sutures and alveolar processes, the mandible will rotate forward.[10] These growth changes significantly alter the lower facial height and the position of the chin horizontally and vertically.
According to Sassouni and Nanda,[5] mandibular growth in open-bite skeletal type is vertical whereas in deep-bite it is predominantly horizontal.
Vertical dysplasia is due to the interaction of many etiological factors during the development of the maxilla and mandible, lips, tongue, and dentoalveolar region.[8]
Mandibular growth and vertical discrepencies
Mandible has direct articulation with the skull, therefore if the vertical growth increases in the anterior face then the same amount of vertical growth increases in the posterior facial height. [11] Understanding the maxillomandibular rotations helps in the diagnosis of vertical variations. Bjork and Skieller[12] conducted a study to demonstrate the direction of growth of the mandible and concluded that the most common direction of condylar growth is vertical. Patients with upward and forward growth of the mandibular condyle are characterized by reduced lower facial height with a deep vertical overbite, deep mentolabial sulcus, and strong overclosed appearance whereas patients with downward and backward growth are characterized by an increase in lower facial height with the most posterior position of chin and sometimes anterior open bite may develop depending on the clinical situation.
Bjork[13] in 1969 has given 7 structural signs of extreme growth rotation in relation to condylar growth direction. They are as follows:
Inclination of the condylar head,
Curvature of the mandibular canal,
Shape of the lower border of the mandible,
Inclination of the symphysis,
Interincisal angle,
Interpremolar or intermolar angles,
Anterior lower facial height
Pearson [14] has given 7 criteria to assess the difference between forward(low-angle) and backward(high-angle) rotators, based on Bjork 7 structural signs ([Table 2]).
Mandible rotates both in a clockwise and counterclockwise direction.[15] These rotations can alter the facial heights as follows:
Clockwise rotation of the mandible is due to excessive vertical growth as it relates to horizontal growth and reduces the vertical overbite.
Counterclockwise rotation of the mandible is due to deficiency of vertical growth as it relates to horizontal growth and increases the vertical overbite.
Etiology of long face
According to Rakosi,[16] the etiology of the open bite can be broadly divided into:-
Epigenetic in nature – Tongue morphology, size and posture, growth pattern of maxilla and mandible
Environmental factors – Respiratory dysfunction
According to Subtnley, [17] 3 etiological factors have been associated with open bite:
Vertical growth deficiencies – vertical deficiency in the anterior portion of the maxilla
Disproportionate muscle growth or aberrant muscle function
Thumb and finger-sucking habits
Etiology of short face
Based on the etiology, deep bite can be divided into developmental deep bite and acquired deep bite. [16]
Developmental deep bite [16]: It is of 2 types
Skeletal deep bite with a horizontal growth pattern
Dentoalveolar deep bite due to supraeruption of incisors.
According to Nanda [2], skeletal deep bite may be caused by either genetic or environmental factors or a combination of both. Other factors include changes in tooth morphology, mesiodistal width of anterior teeth.
Acquired deep bite [16]: Deep bite developed due to environmental factors are known as acquired deep bite. It may occur due to the following reasons:
A lateral tongue thrust or postural position of the tongue results in posterior teeth infraeruption. Example: Class II div 2 malocclusion
Premature loss of primary teeth or early loss of posterior permanent teeth.
Tooth abrasion or occlusal surface wearing.
Diagnostic Considerations of Vertical Discrepencies
A careful differential diagnosis has to be made to assess the long and short face. The clinician must mainly focus on the force systems that are planned for the management of the discrepancies. Inappropriate forces can lead to unwanted problems.[3] Low-angle patients will have strong musculature which will counteract the extrusive forces whereas high-angle patients will have weaker musculature which allows greater expression of the vertical forces.[18] Role of skeletal and dental relationships: Dentoalveolar abnormalities can affect the skeletal pattern and discrepancies in skeletal patterns can affect the dentoalveolar region. These variations can occur alone or in combination: In maxilla - maxillary posterior alveolar excess and inferiorly positioned maxilla, in mandible - mandibular posterior alveolar excess and short mandibular rami. Other conditions like superiorly positioned condylar fossa, obtuse cranial base angle, and condylar resorption. Any of these conditions can be causative factors for the discrepancy in vertical dimension.[3] Diagnosis of the vertical dimension includes a complete examination of the patient. It includes:
Case history
Clinical examination
Radiographs
Study models
Photographs
Management of Vertical Discrepencies
Vertical discrepancies are to be corrected in such a way that the adjustments must be made by favourable growth of the mandible and the alveolus of the mandible and maxilla. A rational approach for planning treatment for a patient with a vertical discrepancy begins with the identification of the dental and skeletal components contributing to the malocclusion in vertical dimensions. Generally, vertical malocclusions are the most difficult to correct. The prognosis of anterior open bite may be either very good when treated at an early age or very poor if the patient exhibits severe discrepancy. For deep bite cases, a good prognosis can be seen with the passing of time.[19]
Management of long face
Management of open bite varies depending on the age of the patient. In growing individuals, the main aim is to control the eruption of molars. Whereas in adults, the vertical excess length can be treated with orthognathic surgery and camouflage treatment depending on the severity of the open bite.[2] The goal of the treatment is to control the vertical development or intrusion of the buccal dentoalveolar region and to allow the forward and upward rotation of the mandible.[2]
Methods to control the open bite in growing patients
Habit breaking appliances: Helps in altering tongue posture which helps in the correction of anterior open bite. A Palatal tongue crib is beneficial in patients with prolonged thumb-sucking habits. Example: Tongue crib ([Figure 6] ), Lingual spurs.[2]
Functional appliances: Uses a series of tongue exercises that help in muscle retraining to correct the abnormal deleterious resting and functional postures. Example: Frankel regulator.[20]
Headgear: Occipital and vertical-pull headgears are the most commonly used extraoral maxillary traction appliances to control the vertical dimension. They exhibit intrusive force on maxillary molars.[21]
Posterior bite blocks: They are passive acrylic functional bite blocks that open the mandible by 3-4 mm beyond interocclusal distance and also it will maintain the pressure which is applied on the posterior teeth by masticatory muscles. Also, spring loaded bite blocks and magnetic bite blocks (active vertical correctors) apply continuous vertical force on posterior teeth occlusal surfaces.[2]
Vertical-Pull chin cup: During the mixed and early permanent dentition period, a vertical pull chin cup is used to control the increase in the anterior facial height.[2]
Masticatory muscle exercises: The contractile force of the elevator muscles of the mandible can be increased with isometric clenching exercise thereby reducing the anterior facial height, gonial angle, and counterclockwise rotation of the mandible.[2]
Vertical holding appliance: It is a modified transpalatal arch introduced by Deberardinis et al,[22] used in high-angle patients to control vertical dimension.
Methods to control the open bite in non-growing patients:
Temporary Anchorage Devices (TADs): In open bite patients, TADs are used for the control of vertical dimension by intruding molars. They reduce the anterior facial height; lip incompetency can be reduced by rotating the mandible counterclockwise ([Figure 7]).[23]
Orthognathic surgery: Patients with vertical maxillary excess can be treated in 3 ways: Superior repositioning of maxilla/mandibular surgery/superior repositioning of chin by a mandibular lower-border osteotomy.[24]
Extractions for open bite closure: Anterior open bite can be closed by extracting different teeth depending on the clinical scenario[2]
Second molar extractions
First molar extractions
Premolar extractions
Management of short face
Treatment by various mechanics
Deep overbite in orthodontics can be corrected by following methods:[25]
Intrusion of anterior teeth






|
Deep bite |
Open bite |
|
Short face syndrome |
Long face syndrome |
|
Concave profile |
Convex profile |
|
Reduced anterior facial height & Increased posterior facial height |
Increased anterior facial height & Reduced posterior facial height |
|
Hypodivergent growth pattern Mandibular rotation-Downward and |
Hyperdivergent growth pattern |
|
Mandibular rotation-Upward and Forward |
Backward |
|
Shorter gonial angle |
Larger gonial angle |
|
Anteriors - Supraerupted Posteriors - Infraerupted |
Anteriors - Infraerupted Posteriors - Supraerupted |
|
Bjork 7 structural signs |
Forward Rotators |
Backward rotators |
|
|
1 |
Inclination of the condylar head |
Curve forward and back |
Straight/slopes up |
|
2 |
Curvature of the mandibular canal |
Curved |
Straight |
|
3 |
Shape of the mandibular lower border |
Curved downward |
Notched |
|
4 |
Inclination of the symphysis |
Slopes backward |
Slopes forward |
|
5 |
Interincisal angle |
Obtuse |
Acute |
|
6 |
Interpremolar or intermolar angles |
Obtuse |
Acute |
|
7 |
Anterior lower facial height |
Short |
Tall |
Combination of Intrusion and Extrusion
Intrusion of anterior teeth
Incisors are intruded in deep bite patients with vertical maxillary excess, a large interlabial gap, a long lower facial height, or a steep mandibular plane. Force should be applied through the centre of resistance of the incisors to avoid their proclination.[26] Anteriors can be intruded by 2 methods: continuous and segmental techniques.
Continuous technique: It includes an increased curve of spee and selective vertical steps in the archwire. Molar extrusion and also buccal tipping can occur with this technique.[25]
Segmental technique: It includes the following appliances:
Rickets utility arch ([Figure 8])
Burstone intrusion arch
Three-piece intrusion arch
The above-mentioned appliances differ in the wire size and material, method of attachment to the brackets, force amounts, and the inclusion of torque within the force system. Additionally, high-pull headgear can also be used to control molar extrusion.[25]
Extrusion of posterior teeth
This is the most common method for the correction of deep bite in patients with short lower facial height, excessive curve of spee, and also incisor exposure.
Various methods are employed for the extrusion of posterior teeth in deep bite patients, including the following:
Placement of anterior brackets more occlusally.[25]
Levelling the arches using the reverse curve of spee wire in the mandible and the exaggerated curve of spee in the maxilla (ROCKING CHAIR).[25]
Bonding of 2nd molars in both the arches.[25]
Inclusion of step bends in the archwires which gradually increase from incisors to premolars.
Anterior bite planes: They can be given as removable or fixed appliances. Bite planes are effective in growing patients particularly on the mandibular arch since they level the mandibular curve of spee. In fixed appliances, the levelling is maintained with stiffer wires in the mandibular arch ([Figure 9]).[25]
Other auxiliaries like bite turbos can also be bonded on the palatal surface of maxillary incisors to separate the posterior teeth ([Figure 10]).[25]
Proclination of incisors
Incisors are to be proclined in cases with lingually tipped incisors (Class II div 2 and Class III malocclusions). Proclination of incisors reduces the amount of overbite.[25]
Combination of intrusion and extrusion
Simultaneous intrusion and extrusion can be performed by placing anterior brackets occlusal and posterior brackets gingivally. And also reverse curve archwires can also be used.[2]
Considerations in growing patients: In growing patients, a removable anterior bite plane can be given for deep bite correction which helps in the eruption of posterior teeth while maintaining the incisor’s heights.[25] Considerations in non-growing patients: In non-growing patients with severe skeletal discrepancy orthognathic surgery is performed since there is no growth left. Extractions are usually avoided in a deep bite patient to overcome the worsening of the bite.[25]
Conclusion
Three-dimensional diagnosis and a good understanding of the interaction between the neuromuscular parts of the orofacial region and craniofacial skeleton help in achieve the ideal treatment outcomes. Control of vertical dimension is important in treating patients with vertical discrepancies. While dealing with these patients, clinicians should remember that all the cases cannot be treated similarly due to extreme variation in facial patterns and morphological characteristics.[6] But in reality, the vertical dimension is the easiest to deal out of all the dimensions since it grows most in magnitude for a longer period.
Conflict of Interest
None.
Source of Funding
None.
References
- S Braun. Biomechanical considerations in themanagement of the vertical dimension. Semin Orthod Elsevier 2002. [Google Scholar]
- R Nanda. . Esthetics and Biomechanics in Orthodontics 2014. [Google Scholar]
- JL Vaden, LE Pearson. Diagnosis of the vertical dimension. Semin Orthod Elsevier 2002. [Google Scholar]
- AJ Haas. A Biological Approach to Diagnosis, Mechanics and Treatment of Vertical Dysplasia. Angle Orthod 1980. [Google Scholar]
- V Sassouni. A classification of skeletal facial types. Am J Orthod 1969. [Google Scholar]
- A Karad. . Clinical Orthodontics: Current Concepts, Goals and Mechanics 2014. [Google Scholar]
- TM Graber, BF Swain. . Orthodontics, Current Principles and Techniques. 1985. [Google Scholar]
- D Ib Leth Nielsen. Vertical malocclusions: etiology, development, diagnosis and some aspects of treatment | The Angle Orthodontist. Angle Orthod 1991. [Google Scholar]
- MH Ortiz, AG Brodie. On the growth of the human head from birth to the third month of life. Anat Rec 1949. [Google Scholar]
- FF Schudy. Vertical Growth Versus Anteroposterior Growth As Related To Function And Treatment. Angle Orthod 1964. [Google Scholar]
- JR Isaacso, RJ Isaacson, W Speidel. Extreme Variation in Vertical Facial Growth and Associated Variation in Skeletal and Dental Relations. Angle Orthod 1971. [Google Scholar]
- A Bjo, V Skieller. Facial development and tooth eruption: An implant study at the age of puberty. Am J Orthod 1972. [Google Scholar]
- A Björk. Prediction of mandibular growth rotation. Am J Orthod Elsevier 1969. [Google Scholar]
- LE Pearson. Vertical Control in Treatment of Patients Having Backward-Rotational Growth Tendencies | The Angle Orthodontist. Angle Orthod 1978. [Google Scholar]
- FF Schudy. The Rotation Of The Mandible Resulting From Growth: Its Implications In Orthodontic Treatment . Angle Orthod 1965. [Google Scholar]
- TM Graber, T Rakosi, AG Petrovic. . Dentofacial Orthopedics with Functional Appliances 1997. [Google Scholar]
- JD Subtelny, M Sakuda. Open-bite: Diagnosis and treatment. Am J Orthod 1964. [Google Scholar]
- B Kusnoto, BJ Schneider. Control of the vertical dimension. Semin Orthod Elsevier 2000. [Google Scholar]
- A Richardson. Skeletal factors in anterior open-bite and deep overbite. Am J Orthod 1969. [Google Scholar]
- R Fränkel, C Fränkel. A functional approach to treatment of skeletal open bite - PubMed. Am J Orthod Dentofac Orthop 1983. [Google Scholar]
- P Brown. A cephalometric evaluation of high-pull molar headgear and face-bow neck strap therapy. Am J Orthod 1978. [Google Scholar]
- M Deberardinis, T Stretesky, P Sinha, RS Nanda. Evaluation of the vertical holding appliance in treatment of high-angle patients. Am J Orthod Dentofac Orthop Elsevier 2000. [Google Scholar]
- YJ Choi, H Suh, JJ Park, JH Park. Anterior open bite correction via molar intrusion: Diagnosis, advantages, and complications. J World Fed Orthod 2024. [Google Scholar]
- LJ Bailey, WR Proffit, GH Blakey, DM Sarver. Surgical modification of long-face problems. Semin Orthod Elsevier 2002. [Google Scholar]
- JG Ghafari, AT Macari, RV Haddad. Deep bite: Treatment options and challenges. Semin Orthod 2013. [Google Scholar]
- R Nanda, SD Kapila. . Current Therapy in Orthodontics 2010. [Google Scholar]
- Introduction
- Development of Vertical Discrepencies
- Diagnostic Considerations of Vertical Discrepencies
- Management of Vertical Discrepencies
- Management of long face
- Methods to control the open bite in growing patients
- Methods to control the open bite in non-growing patients:
- Management of short face
- Combination of Intrusion and Extrusion
- Intrusion of anterior teeth
- Extrusion of posterior teeth
- Proclination of incisors
- Combination of intrusion and extrusion
- Conclusion
- Conflict of Interest
- Source of Funding