- Visibility 23 Views
- Downloads 4 Downloads
- DOI 10.18231/j.idjsr.2023.029
-
CrossMark

Gorlin-goltz syndrome: A case report
Introduction
The Gorlin-Goltz Syndrome (GGS) is inherited autosomal multisystemic disease. It is also known as the nevoid basal cell carcinoma syndrome (NBCCS). In year 1894, the Jarisch and White first describe patients of this syndrome, describing the presence of multiple basal cell carcinomas. In 1960 Gorlin and Goltz established the classical triad which characterizes the diagnosis of this syndrome (multiple basal cell epitheliomas, kerato-cysts in the jaws, and bifid ribs) which were then modified by Rayner et al., should be present odontogenic kerato-cysts in combination with calcification of the falx cerebri or palmar and plantar pits.
It was observed that the wide range of other neurological, ophthalmic, endocrine, and genital manifestations are in association with this triad. Male is to female ratio is equal. Currently, genetic studies point out the markers such as PTCH1, PTCH2, and SUFU which are accountable of syndrome. Out of them, mutation in Patched1 (PTCH1) gene has been identified as the main cause for GGS. [1], [2], [3], [4], [5]
Case Report
An 19 years old, male patient came to Oral & Maxillofacial Surgery department, Rural Dental College, Loni, had given chief complaint of swelling in lower front region of jaw. The duration of the swelling was 3 months & was of slow growing nature. No significant history of tooth ache in same region. No history of pus discharge or bleeding from the lesion.
On examination, well defined extra oral swelling seen on lower one-third of face on the right side. Extending supero-inferiorally from 2.5 cm below ala-tragus line to lower border of mandible and antero-posteriorly from corner of mouth to 4 cm ahead of angle region of mandible. Measuring approximately 3 x 3 cm. Overlying mucosa was normal. On the palpation the swelling was firm in consistency, non-tender, afebrile.
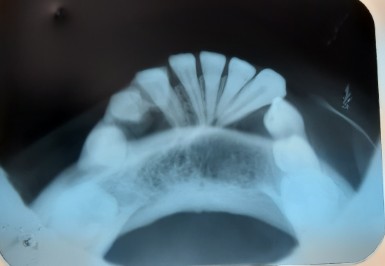
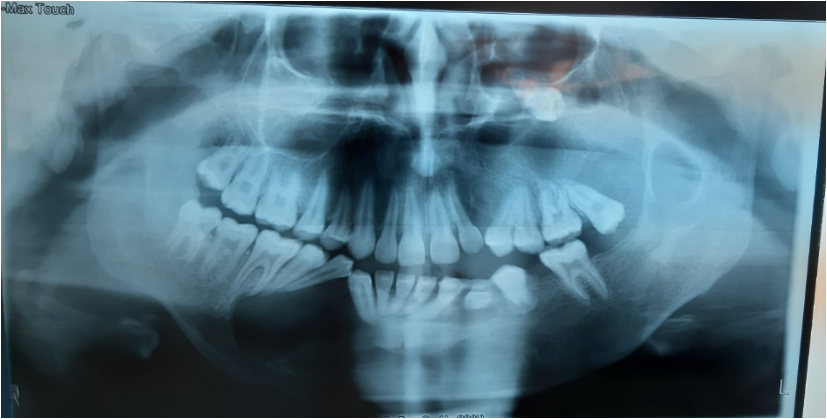
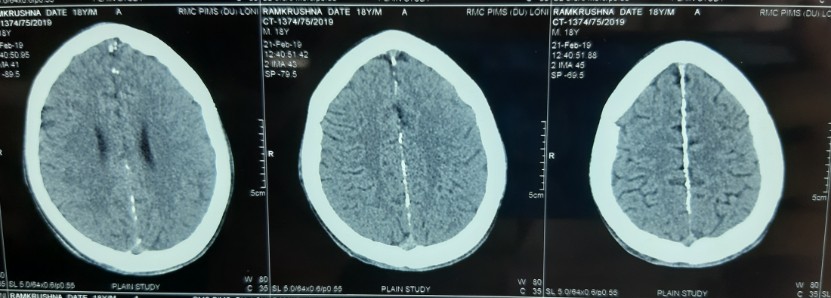
On examination, frontal bossing, broad nasal bridge, hypertelorism noticed. Orthopantomograph showed multiple well - defined multilocular radiolucencies, with presence of sclerotic border in maxilla and mandible. Further, the multiple cysts in the jaws, and the extra-oral examination point out towards Gorlin syndrome and so other confirmatory & relevant investigations were done including Radiographs, CT scan and Histopathological examination.



Flecks and keratin whorls seen in specimen during histopathological examination. There is evidence of cystic lining suggestive of- Odontogenic Keratocyst. Further, enucleation of the cysts was carried out surgically in the Oral & Maxillofacial surgery department, Rural Dental College, Loni. Other skin lesions like basal cell nevus or keratosis were absent.
Based on the clinico-radiographic, & histological findings, with reference of the diagnostic criteria, patient was diagnosed with the GGS.

Discussion
In Gorlin-Goltz syndrome, which is an autosomal dominant inherited syndrome, which involves the skin, nervous system, eyes, endocrine system, and skeleton. The condition is also called as the basal cell nevus syndrome, multiple basal cell carcinoma syndrome, Gorlin syndrome, multiple nevoid basal cell epithelioma-jaw cysts, or hereditary cutaneo-mandibular polyonocosis or bifid rib syndrome. To set up a diagnosis of the Gorlin–Goltz syndrome, the criteria selected were given by Evans et al. (1993), which was later modified by Kimonis et al. (2004). Diagnosis of GGS is confirmed by fulfilling two major and one minor or one major and three minor criteria. [6], [7], [8], [9], [10], [11]
Major criteria for GGS
Basal Cell Carcinoma (multiple or one occurring under the age of 20 years)
Histopathologically proven KCOTs of the jaws
Three or more palmar or plantar pits
Bilamellar calcifications of the falx cerebri
Bifid, fused, or markedly splayed ribs
First-degree relative with GGS.
Minor criteria for GGS
Macrocephaly
Cleft lip or cleft palate and other congenital malformation
Frontal bossing, coarse face, and moderate or severe hypertelorism
Other skeletal abnormalities: Sprengel deformity, marked pectus deformity, and marked syndactyly of the digits
Radiological abnormalities: Bulging of sella turcica, vertebral anomalies such as hemi vertebrae, fusion, or elongation of vertebral bodies, defects of the hands and feet, or flame-shaped hands or feet.
Ovarian fibroma
Medulloblastoma
The Woolgar et al. and Dominiguez et al. reported remarkable distinguishing points between single and syndrome keratocysts. The Syndrome keratocysts had noticeable increase in number of satellite cysts, solid islands of epithelial proliferation, odontogenic rests within the capsule, and mitotic figures in the epithelial lining of the main cavity.
Conclusion
To conclude, GGS is a dominant autosomal genetic disorder, which is needs to be evaluated by Craniofacial health experts. Early diagnosis of the condition is important for counselling of patients to avoid harmful exposure from UV and ionizing radiations which increase the chances to develope Basal Cell Carcinoma. For the early diagnosis of GGS, experts should suggest clinico-radiographic examinations in early stages of life.
Source of Funding
None.
Conflict of Interest
None.
References
- OG De Amezaga, OG Arregui, SZ Nuño,, AA Sagredo, JMA Urizar. Gorlin-Goltz syndrome: clinicopathologic aspects. Med Oral Patologia Oraly Cirugia Bucal 2008. [Google Scholar]
- K Patil, VG Mahima, B Gupta. Gorlin syndrome: A case report. J Indian Soc Pedodontics Prevent Dent 2005. [Google Scholar]
- DS Jawa, K Sircar, R Somani, N Grover, S Jaidka, S Singh. Gorlin-Goltz syndrome. J Oral Maxillofacial Pathol 2009. [Google Scholar]
- DGR Evans, EJ Ladusans, S Rimmer, LD Burnell, N Thakker, PA Farndon. Complications of the naevoid basal cell carcinoma syndrome: results of a population based study. J Med Genet 1993. [Google Scholar]
- VE Kimonis, AM Goldstein, B Pastakia. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet 1997. [Google Scholar]
- M Kohli, M Kohli, N Sharma, SR Siddiqui, SPS Tulsi. Gorlin-Goltz syndrome. National J Maxillofacial Surg 2010. [Google Scholar]
- RJ Gorlin, MM Cohen, RCM Hennkem. . Hennkem, Syndromes of Head and Neck. 4th Edn. 2001. [Google Scholar]
- JA Woolgar, JW Rippin, RM Browne. A comparative histological study of odontogenic keratocysts in basal cell naevus syndrome and control patients. J Oral Pathol 1987. [Google Scholar]
- FV Dominguez, A Keszler. Comparative study of keratocysts, associated and non-associated with nevoid basal cell carcinoma syndrome. J Oral Pathol 1988. [Google Scholar]
- S Rai, K Gauba. Jaw cyst-Basal cell nevus-Bifid rib syndrome: a case report. J Indian Soc Pedodontics Prevent Dent 2007. [Google Scholar]
- L Lo Muzio. Nevoid basal cell carcinoma syndrome (Gorlin syndrome). Orphanet J Rare Dis 2008. [Google Scholar] [Crossref]