Introduction
Facial esthetics plays a very important role in the field of dentistry. During a usual examination, impacted teeth may not be always detected. Impacted or clinically missing permanent incisors have a major impact on the dentofacial aesthetics of an individual. The reasons for such missing can be due to supernumerary teeth, malposition, Ankylosis, odontomas or in diseases like Cleidocranial dysostosis, Hypopituitarism and Ectodermal dysplasia.
Odontomas are generally non-aggressive, hamartomatous lesions of enamel, dentin, cementum, or pulp tissue of odontogenic origin.1 Dentin and enamel can be deposited in odontomas in a manner that gives them anatomical similarities to normal teeth.2 In routine radiographic examinations, odontomas are usually found as small, solitary, or multiple radio-opaque lesions.3
Traditionally odontomas have been classified as benign odontogenic tumors and are subdivided into complex or compound odontomas morphologically.
Compound odontomas commonly occur in the maxilla’s incisor-canine region, and complex odontomas are frequently located in the premolar and molar regions of both jaws. Frequently, they interfere with the eruption of the teeth.4 Radiographically, compound odontomas are characterized by multiple irregular radio-opaque lesions that vary in size and shape and contain tooth-like structures called denticles, whereas complex odontomas manifest as a radiopaque solid mass with occasional nodular elements and are surrounded by a fine radiotransparent zone. It is a unilocular lesion distinguished from the normal bone by a well-defined corticalization line. 5, 6 The exact etiology of an odontoma is unclear,6 although local trauma, infection, hereditary anomalies, odontoblastic hyperactivity, or alterations of the genetic components are responsible for controlling tooth development. There is No gender predilection, but According to Budnick, males were more likely to suffer from the disease (59%) than females (41%), and it was mainly seen in the first two decades of life.
Case Description
A 10-year-old girl visited the Dept of Pediatric and Preventive Dentistry, with a chief complaint of missing teeth in the upper front tooth region. There is no history of pain or trauma. There is no family history of unerupted teeth
The child had a mixed dentition. The patient had a habit of tongue thrusting. During the soft tissue examination, a noticeable and firm bulge measuring 1cm*1cm was observed in the anterior maxillary region. Notably, there was no tenderness upon palpation, and there was no presence of purulent discharge. This finding suggests the absence of any acute infection or inflammation in the area.

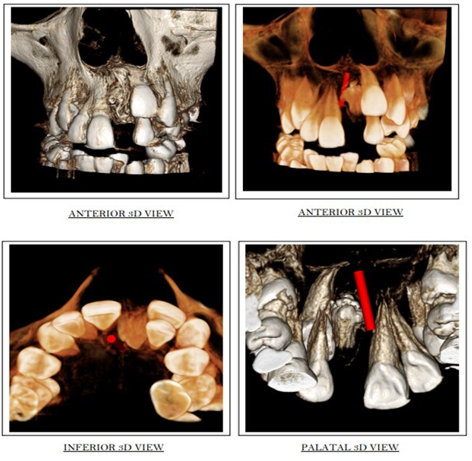
As a part of the investigation, CBCT was taken and the report revealed a mixed radiolucent and radio-opaque lesion of variable density resembling a tooth-like structure, with a radiolucent peripheral rim and well-defined dense cortical border, located in the anterior maxilla at the native position of 21. The mixed radiopaque lesion is occupying almost the entire alveolar process. The lesion is located between 11 and 22 anteriorly. It is in contact with the lateral border of the incisive canal. As per the CBCT report lesion roughly measures about 8.9 mm mesiodistally and 13.4 superior inferiorly and there is thin bone covering both the labial and palatal aspects of the lesion. The permanent central incisor 21 remained impacted and is located partly anterior to the radiopaque lesion and partly anterior to the position of 21. CBCT investigation suggested the diagnosis as compound odontoma.
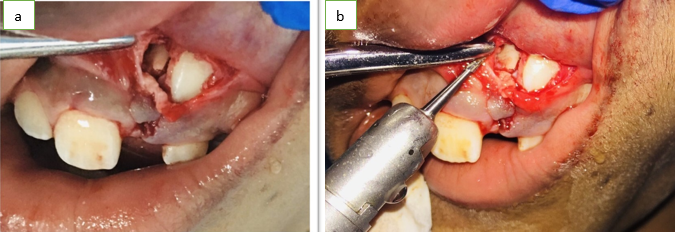
The procedure began with the administration of a local anesthetic solution to ensure the patient's comfort. Following this, both horizontal and vertical incisions were made to access the affected area properly. The dental flap was then elevated to expose the calcified tooth-like structures, which were surgically removed. After the successful removal of the calcified structures, the wound was carefully closed using 3-0 silk sutures to promote proper healing. This comprehensive approach aimed to address the condition effectively and promote favorable postoperative outcomes for the patient.

Gross examination showed a miniature teeth-like structure. The sample collected was sent to the Department of Oral Pathology for histopathological examination.
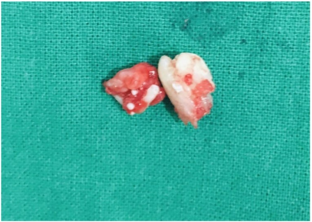
Figure 6
Histopathological section of specimen showing irregular arrangement of fibers with focal area of hyalinization and a few calcified masses
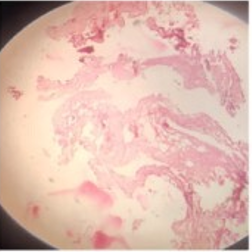
Decalcified sections of miniature tooth-like structures ground section showed the regularly arranged dental hard tissue resembling the tubular dentin and cementum. (Figure 7)
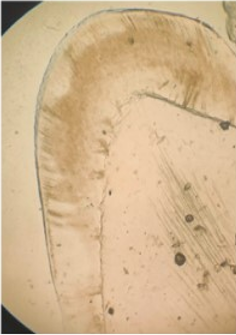
The histopathological examination confirmed the diagnosis of a compound odontoma.
Discussion
Odontoma frequently encountered, are asymptomatic odontogenic hamartomatous malformations often found in connection with impacted or retained primary teeth. 7
The mean age of detection on average is 14.8 years, with the prevalent age being the second decade of life.
According to Owen et al, Yaseen et al there is a slight predilection for the occurrence in males compared to females. The compound odontome is known to occur more commonly in the maxilla (67%) than the mandible (33%), with a marked predilection for the anterior maxillary region (61%). 8, 9
In 1914, Gabell, James, and Payne grouped odontome according to their developmental origin: epithelial, composite (epithelial and mesodermal), and mesodermal. 10
In 1946, Thoma and Goldman gave a classification which is as follows: 11
Geminated composite odontomes: A combination of two or more well-developed teeth
Compound composite odontomes: Made up of more or less rudimentary teeth
Complex composite odontomes: Calcified structure bearing little resemblance to the dental tissues in their normal arrangement
Dilated odontomes: The crown or root part of tooth shows a marked enlargement
Cystic odontomes: It is normally enclosed by fibrous connective tissue within a cyst or in its wall.
According to the World Health Organization (WHO) classification, odontomes can be divided into three groups: 12
Complex odontome: when the calcified dental tissues are simply arranged in an irregular mass bearing no morphologic similarity to rudimentary teeth.
Compound odontome: composed of all odontogenic tissues in an orderly pattern, which result in many teeth-like structures, but without morphological resemblance to normal teeth.
Ameloblastic fibro-odontome: consists of varying amounts of calcified dental tissue and dental papilla-like tissue, the later component resembling an ameloblastic fibroma. The ameloblastic fibro-odontome is considered as an immature precursor of complex odontoma.
Compound odontomas are characterized by high morphologic differentiation, producing many tooth-like structures. 13
The diagnosis is usually established on the basis of routine radiological examination (panoramic and/or intraoral radiographs), or on evaluating the cause of delayed tooth eruption. 14
The treatment of choice is the surgical removal of the lesion in all cases, followed by a histopathological study to confirm the diagnosis.
There is a small probability of recurrence of odontomas after conservative surgical removal. 15 Timely detection and surgical enucleation of odontomas followed by curettage are recommended to prevent complications such as tooth loss, cystic changes, bone expansion, and delayed eruption of permanent teeth. 16
Conclusion
Odontomas seldom emerge into the mouth due to their tendency to be associated with impacted and retained teeth. Every pediatric patient with clinical evidence of delayed eruption or missing teeth should undergo a thorough visual examination, manual examination, and radiographic examination. Early detection permits the adoption of a less complex and more cost-effective treatment approach, leading to improved outcomes.