- Visibility 478 Views
- Downloads 34 Downloads
- Permissions
- DOI 10.18231/j.idjsr.2023.016
-
CrossMark

Correction of anterior and lingual single tooth cross bite in an adult patient - A case report
- Author Details:
-
 Sushmita Batni Rao *
Sushmita Batni Rao *
-
Vikram Shetty
-
Taher Manasawala
-
Devashree Mujumdar
Abstract
Malocclusion is known to be multifactorial affecting a wide range of populations in many ways. It can have pernicious effects on the quality of life of an individual since it is associated with both aesthetic and functional matters. Crossbites, having been considered one of the most common malocclusions, also serves as a route for future problems. The objective was to treat a 22-year-old male patient who presented with a single tooth anterior and lingual crossbite. A non-extraction treatment followed by settling of occlusion which met the treatment plan was performed, delivering a corrected smile both functionally and aesthetically.
Introduction
Crossbite can be defined condition where one or more teeth may be abnormally malposed buccally or lingually or labially with reference to the opposing tooth or teeth (Graber, 1994).[1] Many studies have stated that the incidence of crossbites varies between 1-23%, of which around 6-7% constitute single tooth crossbites, 4-5% of unilateral crossbites, and around 1-3% constitute bilateral crossbites.[2] According to the region, crossbites can be classified into anterior or posterior crossbites. Anterior crossbite is said to be caused when the maxillary incisors occlude lingually to the mandibular incisors. Whereas Posterior crossbite is said to be caused due to an abnormal transverse relationship between the maxillary and mandibular posterior teeth where the maxillary posterior teeth occlude either buccal or lingual to the mandibular posterior teeth.[3]
Anterior or Posterior crossbites can occur due to various causes such as delayed shedding of the corresponding primary tooth, incisor crowding, arch length discrepancy, or trauma to the primary tooth leading to a change in the eruption pathway of the permanent tooth.[4] Crossbites correction is indicated in early stages (early mixed dentition) to prevent any hindrance to the normal growth of both jaws and to avoid the occurrence of neuromuscular disturbances in the temporomandibular joint function due to jaw asymmetry or any functional displacement of the mandible. Crossbites may lead to permanent dental, skeletal or functional dissension and may increase the risk of permanent temporomandibular disproportion in the future if left untreated.[5]
A 22-year-old male patient reported to the Department of Orthodontics with a chief complaint of malaligned teeth in the upper front region. He was diagnosed with a Class I skeletal pattern with orthognathic maxilla and mandible and an average growth pattern. The patient had a Class I molar relationship bilaterally. Crossbite was present with 21 and 35, followed by mild lower anterior crowding. Midlines were coincident. The patient had a straight profile, obtuse nasolabial angle with everted competent lips. The upper and the lower 3rd of the face were not correlated to each other since there was an upper lip deficiency. ([Figure 1], [Figure 2])
The patient refused to undergo extraction of any teeth; therefore, the following treatment plan was established:
Attachment of brackets and bands followed by leveling and aligning of both the arches.
Maintenance of space between 11 and 22 and 35 and 36 for correction of crossbite of both teeth.
Temporary disocclusion by the placement of bite turbos over the maxillary posterior teeth.
Correction of crossbite followed by settling of occlusion.
The treatment plan was explained, and an informed consent was taken from the patient. All the teeth were bonded except 21 and 35. After a few months of levelling and aligning all the teeth, the treatment progressed where a base arch wire of 0.017 X 0.025 Inch Stainless Steel was placed in both the arches.
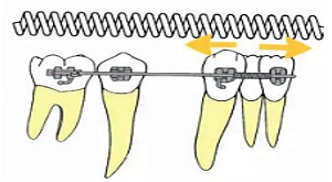
A Nickel Titanium Open Coil spring was placed between 11 – 22 and 34-36 to maintain the gap for correction of the crossbite with respect to 21 and 35. After 6 months of the leveling and aligning phase, both 21 and 35 were bonded and a 0.014-inch Nickel Titanium wire was placed as a “Piggyback” to get them into occlusion. ([Figure 3])
Simultaneously, the posterior teeth were disoccluded by using bite turbos on the maxillary 1st permanent molars so that it could initiate faster correction of the teeth in crossbite without any occlusal interference. Both the anterior and lingual crossbites were corrected within 3-4 months after which the occlusion was settled using settling elastics.
Results
The result after 15 months of treatment showed a corrected crossbite occlusion with a well-maintained molar relationship bilaterally and coinciding midlines intraorally. The patient’s profile was maintained followed by a decent smile. ([Figure 4], [Figure 5])




Discussion
Treatment of crossbites in the early stages, especially during the mixed dentition stage, aims to tap the affected teeth labially where a stable overjet and overbite relationship exists during occlusion. When this is achieved, there are great chances of prevention of relapse. [6]
Lee et al [7] in their study stated that the following four factors have to be considered before selecting any treatment approach;
Adequate space present in the arch for repositioning the tooth
Apical position of the tooth in crossbite coincides with that of the teeth in occlusion.
Adequate overbite to avoid relapse.
Class I occlusion for long term stability.
Early treatment of anterior dental crossbites can be achieved by several methods such as; [8]
Tongue blade therapy
Lower inclined plane
Stainless Steel crowns
Hawley retainer with auxiliary spring
2x4 fixed appliance
Treatment of crossbites in adults becomes comparatively difficult since the occlusion is set during the growing stages and more force is required to tip the teeth labially as compared to the mixed dentition period. Since the teeth must be disoccluded for a significant amount of time, it becomes difficult for the patient to manage the day-to-day routine and may also interfere with speech.
Ngom and Coll [9] in their study stated that there is a correlation between anterior crossbite, and gingival recession of the corresponding tooth, and the primary cause could be occlusal trauma. Such scenarios can be seen in anterior crossbite cases where gingival recession can be observed in the lower incisor after the correction. This may be because the apical portion of the alveolar ridge has the least thickness which could lead to recession.
The use of fixed appliance in this case consisted of preadjusted MBT brackets and are known to have a few advantages such as their versatility and provision of light continuous force. Since there was inadequate space for the incisor and premolar to be brought into the arch, the use of NiTi coil springs had the main advantage. These springs exhibit excellent spring back properties as well as deliver a continuous force due to their large range of superelasticity with a constant load over a large deflection. [10]
Conclusion
Treatment of crossbites, even though sounds easy but becomes particularly challenging to the clinician sometimes. Maintenance of a proper occlusion after the correction is extremely pretentious, especially in cases such as the one explained above. The outcome of the treatment consummates the given treatment plan, therefore, considering it as a success. The patient is completely satisfied with the results of the treatment from both the aesthetic and the functional point of view.
Conflict of Interest
None.
Source of Funding
None.
References
- Graber TM, Vanarsdall-Jr R, . . Diagnosis and Treatment Planning in Orthodontics, Orthodontics-Current Principles and Techniques. 1994. [Google Scholar]
- Hannuksela A, Väänänen A. Predisposing factors for malocclusion in 7-year-old children with special reference to atopic diseases. Am J Orthod Dentofacial Orthop. 1987;92(4):299-303. [Google Scholar] [Crossref]
- Sarver D, Proffit W, Ackerman J, TG, RV. Diagnosis and treatment planning in orthodontics. Orthodontics, Current Principles and Techniques. 3rd edn.. 2000. [Google Scholar]
- Bayrak S, Tunc E. Treatment of anterior dental crossbite using bonded resin-composite slopes: Case reports. Eur J Dent. 2008;2(4):303-6. [Google Scholar]
- Iodice G, Danzi G, Cimino R, Paduano S, Michelotti A. Association between posterior crossbite, skeletal, and muscle asymmetry: a systematic review. Eur J Orthod. 2016;38(6):638-51. [Google Scholar]
- Jacobs S. Teeth in cross-bite: The role of removable appliances. Aust Dent J. 1989;34(1):20-8. [Google Scholar] [Crossref]
- Lee B. Correction of crossbite. Dent Clin North Am. 1978;22(4):647-68. [Google Scholar]
- Purcell PD. The crossbite. J Michigan Dent Assoc. 1984;66(2):69-73. [Google Scholar]
- Ngom PI, Diagne F, Benoist HM, Thiam F. Intraarch and interarch relationships of the anterior teeth and periodontal conditions. Angle Orthod. 2006;76(2):236-42. [Google Scholar]
- Miura F, Mogi M, Ohura Y, Karibe M. The super‑elastic Japanese NiTi alloy wire for use in orthodontics. Part III. Studies on the Japanese NiTi alloy coil springs. Am J Orthod Dentofacial Orthop. 1988;94(2):89-96. [Google Scholar]