- Visibility 43 Views
- Downloads 9 Downloads
- DOI 10.18231/j.idjsr.2022.012
-
CrossMark

Evaluation of the microleakage in class II cavities restored with composite resin by using different placement techniques and light cure units– An in vitro study
Introduction
Composite resin restorations are being increasingly used as the first choice restoration/replacement material for failed or unaesthetic amalgam restorations in the interest of aesthetic dentistry. Although mechanical and physical performance, such as wear resistance and aesthetics of composites have improved, polymerization shrinkage remains a challenge. It causes dimensional changes in restoration that result in microleakage at the margins of restoration, and it is a matter of concern for the clinician.[1]
The shrinkage of light cure resin composite restorations will lead to marginal failures, especially at gingival margins, and would cause dentinal hypersensitivity, secondary caries, and pulpal inflammation. [2]
To restore class II cavities, Bulk fill & Packable composites are recommended because of their time-saving and speed of restoration. These materials have high reactivity to light, so insertion in a 4-mm bulk was possible.[3] Disadvantages of Bulk fill & Packable composites is the presence of voids, difficulty in making tight contact restorations with the adjacent tooth, high opacity, and surface roughness.[4] To overcome the shortfalls of Bulk fill & Packable composites, a New type of nanofiller optimized hybrid universal composite Tetric N-Ceram Bulk Fill (TC) was introduced to restore class I & class II cavities. This Composite contains 21% resin matrixes that include Bisphenol A-diglycidyl Dimethacrylate (Bis-GMA), Bis-Ethoxylatedbisphenol (Bis-EMA), and Urethane dimethacrylate (UDMA).[5]
Conventional light curing agent Quartz tungsten halogen (QTH) is considered the standard protocol for curing composite resins. Because of longer curing times, heat production, and degradation of light filament produce an inadequate output of wavelength, hamper composite setting. To overcome these shortfalls of QTH, Light-emitting diode (LED) curing light was introduced which became popular because of, less heat emission and constant wavelength emission when compared to traditional QTH. [6]
The purpose of this in-vitro study is to evaluate post thermocycling microleakage scores in class II cavities restored with Tetetric n ceram (TC) by Bulk fill technique, Incremental technique, Centripetal techniques, followed by polymerization light source QTH and LED.
In this study, the null hypothesis tested was, that nanofiller optimized universal bulk-fill composite, placement techniques, or light sources do not have any effect on gingival marginal micro-leakage scores in class II cavities after thermocycling.
Materials and Methods
This in vitro study was conducted in the Department of Conservative Dentistry and Endodontics and Department of Oral pathology, G. Pulla Reddy Dental College and Hospital, Kurnool.
Inclusion criteria
Extracted maxillary premolar teeth.
Non-carious teeth
Exclusion criteria
Teeth with a fracture or a restoration.
Teeth with developmental anomalies.
Teeth with preparation depths below CEJ.
All teeth are then placed in 3% NaOCl for 24 hours for surface disinfection and then stored in distilled water at room temperature until use.
Methodology
Class II Conventional Mesioocclusal (MO) cavities were prepared with occlusal gingival depth 1mm above the CEJ. The final preparation has the following dimensions, 3 mm – buccolingual extension,
1.5 mm –axial depth
4 mm –occlusocervical extension
Teeth were randomly selected in 3 groups and 20 specimens in each group. The samples will be etched and rinsed, and then a universal matrix will be placed after that the bonding agent will be applied and cured as per described below. These steps are common to all groups.
A universal matrix was placed and adapted to cavosurface margins. This universal matrix band allowed proximal wall reconstruction and reduced the chance of composite overhangs.
Bonding procedure
The cavities were etched with N-ETCH Etchant (37% PHOSPHORIC ACID) for 15 seconds and washed with water for 15 seconds and excess moisture was dried by a foam pellet. TETRIC-N-BOND was applied with an applicator tip and light-cured for 20secs. During the curing of samples, light intensity was checked using a radiometer. Later all specimens were randomly divided into three groups, each containing 20 teeth.
Group I-Bulk Technique
Group II- Incremental Technique with oblique laying
Group III-Centripetal Technique
Restorative procedure
The teeth were restored using composite placement instruments. The techniques is as follows.
Group I: Samples were restored with the bulk-fill technique. A single layer of composite was applied to fill the preparation up to the cavosurface margin. The increment was cured for 40 seconds.
Group II: Samples were restored with the incremental technique with oblique laying. The first increment was horizontally placed at the cervical wall and light-cured for 40 seconds. The second increment was obliquely placed contacting the buccal, and axial walls were cured for 40 seconds. The third increment was obliquely placed, filling the preparation, and light-cured for 40 seconds.
Group III: Samples were restored with the centripetal technique. A thin layer of composite, 0.5mm thick, was applied toward the metallic matrix contacting the cavosurface of the proximal box up to half of occlusal -cervical extension. A second layer was applied over the previous increment contacting the cavosurface margin of the proximal box and forming a marginal ridge. Both the composite increments were cured for 40 seconds. The resulting class one cavity was restored in 2 horizontal increments, each increment being cured for 40 seconds.[7]
Group I (BU): Composite restoration will be placed using the BULK FILL technique. This group was further divided into two subgroups: Group I A represent BU-QTH and Group I B represents BU-LED.
Subgroup IA: (BU-QTH): All specimens will be restored with composite using BULK FILL TECHNIQUE and light-cured with a QTH curing unit.
Subgroup IB: (BU-LED): All specimens will be restored with composite using BULK FILL TECHNIQUE and light-cured with LED curing unit.
Group II(IN): Composite restoration will be placed using Incremental Technique with Oblique Laying. This group is further divided into two subgroups. Group II A represents IN-QTH and Group II B represents IN-LED.
Subgroup IIA: (IN-QTH): All specimens will be restored with composite using Incremental Technique with Oblique Laying and cured with a QTH curing unit.
Subgroup IIB: (IN-LED): All specimens will be restored with composite using INCREMENTAL TECHNIQUE WITH OBLIQUE LAYING and cured with LED curing unit.
Group III(CE): Composite restoration will be placed using Centripetal Technique. This group is further divided into two subgroups. Group III A. represents (CE-QTH), and Group III B. represents (CE-LED)
Subgroup IIIA: (CE-QTH): All specimens will be restored with composite using Centripetal Technique and cured with QTH curing.
Subgroup IIIB: (CE-LED): All specimens will be restored with composite using CENTRIPETALTECHNIQUE and cured with LED curing unit.
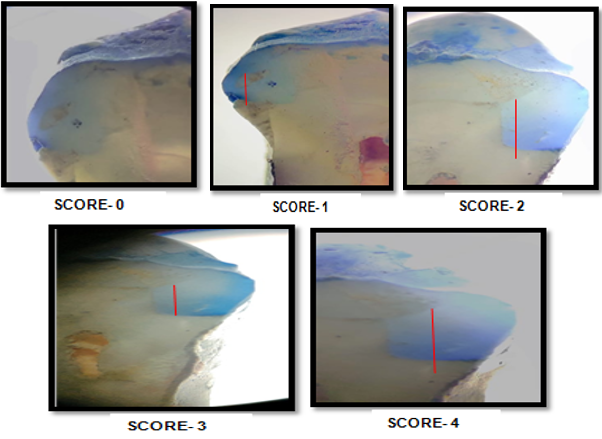
All the specimens, after the restoration was completed, the metallic matrices were removed, and specimens were stored in distilled water at 37˚ C for 24 hours. The restorations were finished and polished by using mani fine diamond burs. specimens were stored in distilled water at 370C till it is subjected to thermocycling. And specimens were thermo cycled for 500 cycles at with temperature range of 5 to 55 degrees with 20 seconds dwell time. To evaluate micro leakage, the teeth surfaces were isolated with 2 layers of fingernail varnish, except for 1 mm around the restoration. Then specimens were immediately immersed in methylene blue dye for 24 hours. Specimens were sectioned along the long axis in the mesiodistal direction of the restoration with a diamond disc and analyzed using a stereomicroscope at 10x magnification by an independent examiner who was blinded by the groups. Scored for the degree of dye penetration along the gingival margins using the scores described below-
Score 0 = no dye penetration.
Score 1 = dye penetration into half of the enamel.
Score 2 = dye penetration into more than half of the enamel.
Score 3 = dye penetration into dentin without extending into the axial wall.
Score 4 =dye penetration into the axial wall.

Results
In the present study, three composite placement techniques (bulk-fill technique, incremental technique, centripetal technique) and two different light-curing units (QTH, LED) were used to evaluate the amount of gingival marginal microleakage using dye penetration technique under a stereomicroscope. Comparison of three groups with microleakage scores at gingival margins by Kruskal Wallis one-way ANOVA test. Pair-wise comparison of all groups with respect to microleakage scores at gingival margins by Mann-Whitney U test. Statistical analysis was performed using SPSS STATISTICS 21.0 software. There was a statistically significant difference among the three groups with the least microleakage seen in incremental technique followed by centripetal and bulk techniques. The mean microleakage values were lowest noticed in group IIB with (0.9± 0.0.8) and the highest values were observed in group IA (2.8± 1.14). With respect to six sub-groups least microleakage was seen with group IIB (IN-LED) followed by group IIA (IN-QTH) followed by group IIIB (CE-LED) followed by group IIIA (CE-QTH) followed by group IB (B-LED) followed by group IA (B-QTH)([Table 1]). There was a statistically significant difference noticed among all six experimental subgroups (P < 0.05).
|
Group |
Mean |
SD |
Median |
Sum of ranks |
|
Group IA |
2.5 |
1.14 |
3 |
421.5 |
|
Group IB |
2.5 |
1.27 |
3 |
421.5 |
|
Group IIB |
1.3 |
1.16 |
1 |
227.5 |
|
Group llA |
0.9 |
0.88 |
1 |
227.5 |
|
Group lllA |
2.2 |
1.23 |
2.5 |
345 |
|
Group IIIB |
1.7 |
1.34 |
1.5 |
278.5 |
Discussion
One of the most disadvantages of resin composites is polymerization shrinkage, which will result in microleakage. Polymerization shrinkage is a complicated process depending on several factors. The volumetric contraction causes debonding forces at the material/tooth interface. The stress resulting from this shrinkage is associated with an open margin between the tooth and the restoration, overt tooth straining or fracture, and post-operative sensitivity. Thus, different techniques have been proposed to improve the marginal adaptation, such as the incremental build-up of the restoration in class II.[8] The cavity configuration (C factor) is one of the several factors that determine the magnitude of shrinkage stresses. The C-factor defines the ratio of bonded to unbounded surfaces. A high ratio denotes high polymerization stresses. Increasing shrinkage stresses accompany it. Extensive efforts made to reduce these stresses. All of them are directed at improving composite resin formulation, curing methods, and restorative placement techniques.[9]
Microleakage assays gave useful information on the performance of restorative materials. Different techniques for assessing microleakage tests developed and used. These tests which use dyes, radioactive isotopes, air pressure, bacterial activity, neutron activation analysis, scanning electron microscope, dye penetration, and microcomputed tomography (μCT) all come with both advantages and drawbacks. The staining of microleakage and nano-leakage using colored agents are the most commonly used technique. The dye penetration process involves the use of contrasting dyes as a concentration solution to stain the area of microleakage, and then the tooth–restoration interface is examined for verification of staining. Notably, the most commonly used solutions are 2% methylene blue, 0.5% basic fuchsin, and 50% silver nitrate. In the present study, methylene blue dye was used because it has many advantages over other techniques. First, no reactive chemicals are used, along with no radiation. Second, the method is highly feasible and easily reproducible.[10]
In the thermal cycling, the extreme differences in temperature, compatible with the ones of the oral cavity, induce differences in expansion and contraction of the restorative material and dental structure leading to percolation" and, therefore, micro infiltration. Thermal cycling influences the marginal infiltration of restoration that has a high coefficient of linear expansion and high thermal infusibility, which promotes the contraction and development of the restoration in a different way than when it occurs in the dental structure. It is suggested that thermal cycling affects the influence of the microleakage of composite resin, even though it may not replicate the exact intraoral conditions. So in our study, we used a dwell time of 20 seconds and 500 thermal cycles.[11]
TETRIC N BOND nano-filled single-component adhesive used in conjunction with the total-etch procedure. The best partner for Tetric N-Bond is the phosphoric acid gel N-Etch same was followed in our study. Tetric N-Bond is used in the position of direct composite and compomer restorations as well as in the adhesive luting of indirect restorations made of all-ceramic and composite materials involving light-curing. A reduced microleakage score has been reported when using filled adhesives in studies by Deliperi S et al. [12]
Along with the placement techniques, even the restorative material used also affects the polymerization shrinkage in the restorations. In our study, we used universal Nanocomposite TETRIC N CERAM for restoration, which Tetric N-Ceram is a light-curing, radiopaque nano-hybrid composite material based on nano-optimized technology for direct restorative procedures. It can be universally applied to restore both anterior and posterior regions. It is responsible for the material's unique chameleon effect and natural esthetic results. Tetric N Ceram Bulk Fill represents the medium viscosity type bulk fill. Curing depth of 4 mm is achieved primarily due to the patented photoinitiator, Ivocerin, which is far more reactive than conventional initiators. The stiffer composites help in restoring useful contacts in posterior teeth. As the filler particle diameter in Nanocomposite was only 5 µm, i.e., about half the wavelength of the activating light and the light scattering was increased, thereby decreasing the degree of conversion and consequently polymerization shrinkage.
Bulk fill RBC materials have been introduced to help dentists reduce placement time and work more efficiently. Manufacturers make claims of these products can fill a cavity in a single 4mm-6mm thickness placement instead of 2 mm thick increments with conventional RBCs. A study conducted by Julian G. Leprince et al. evaluated the physicomechanical properties of most currently available bulk-fill composites. The author finally concluded that the reduction of time and improvement of convenience associated with bulk-fill materials is a definite advantage of this particular material class over conventional composite. [7] Therefore, this bulk fill material was selected for the current study for comparison of the marginal gingival adaptation with different composite placement techniques.
Various placement techniques have been introduced such as oblique incremental, and centripetal increment techniques to reduce C-factor. [13] In the current study, the methods mentioned earlier have been carried out, and the microleakage scores were compared with the bulk placement technique. The results demonstrated that all incremental methods showed a significant reduction in microleakage when compared to bulk. As placing composite in increments reduces the overall volume of composite and reduces polymerization shrinkage. It was also observed from the values obtained with oblique and centripetal techniques showed a significant reduction in microleakage when compared to the bulk technique. Because of layering resin composites have been shown to reduce stresses generated on cavity walls. The reason for lesser microleakage with incremental techniques in our present study may be a result of the low configuration factor. Consequently, minimal shrinkage occurs within each increment. Incremental restoration techniques lower the C-factor to less than 1.0 because there is usually almost as much free surface as a bonded surface in any single increase. E Ozel also stated that the incremental placement technique is the preferred restorative technique for posterior composite restorations as it results in good marginal adaptation. [14]
The oblique technique proposed by Lutz et al. in 1986, was modified in the present study by the use of a metallic matrix instead of a transparent one. The idea of the oblique technique relies on placing small amounts of composite, which increases the adhesive-free surfaces, allows a better flow of the resin, and reduces the shrinkage to a low volume. This procedure minimizes the configuration factor (C-factor) of the preparation, assisting in the adaptation of the composite to the bonded surfaces.[14] The oblique technique is accomplished by placing a series of wedge‑shaped composite increments. Each increment is photocured twice, first through the cavity walls and then from the occlusal surface, to direct the vectors of polymerization toward the adhesive surface. This technique reduces the C‑factor and prevents the distortion of cavity walls. [15]
The incremental oblique layering placement of light-activated composites has been recommended to decrease overall contraction and residual stresses at the tooth or restoration interface and thus decrease microleakage by reducing the bulk of material cured at one time. Similar results were found in studies by tjan et al., supporting the findings in our study significantly. [16] All composite increments were entirely standardized; the horizontal technique would possibly show less microleakage. However, standardized increments are unachievable clinically. Studies have shown that the incremental technique especially the oblique technique tends to improve marginal adaptation by resisting resin composite shrinkage stress. [17] The incremental placement technique has mostly been recommended because it would minimize polymerization contraction and hence, the stresses produced at the bonding interface. When small increments are placed and light-cured, the C factor is reduced. Moreover, the light may adequately reach the deepest composite layers and lead to more significant polymerization, thus minimizing possible marginal degradation that might occur if polymerization was incomplete. [18]
In group III, teeth were restored with the centripetal technique. The primary purpose of the incremental centripetal method is to transform a Class 2 into a Class 1 preparation. In this placement technique, first, a proximal wall is built adjacent to the matrix band converting class II into class I, and later is restored with horizontal increments. Because the amount of composite required to build up the proximal wall is minimal compared to that for the oblique technique, it is supposed to achieve a better marginal adaptation. Besides, it is possible to check the proximal contacts clinically before completing the placement of the increments and correct the proximal contact if necessary.[19] The results of the study are in agreement with the findings of Szep et al. stated that even if there was a gap at the cervical wall after the proximal wall was complete, the following horizontal incremental technique would be able to flow and fill the space. [20]
With the use of the centripetal technique, the V/A ratio could be reduced. This differs from the oblique technique in that the apical area of the cavity will be filled with the first layer of composite resin material. On the contrary, the first layer of the centripetal technique has no contact with the pulpoaxial walls, and thus it has less tendency to contract towards this wall and away from the cervical floor during polymerization. In the proximal box, the polymerization shrinkage tends to pull this first increment away from the cervical margin. The second layer in the oblique, which is diagonal, will not be able to cover the first increment in the cervical area, which can occur with the second layer of the centripetal build-up technique. It is possible that the above-said explanation could be partly responsible for reduced microleakage scores of the centripetal [7] technique as compared to the oblique technique, as seen in our study. However, the results were not statistically significant among both groups. Similar results were found in studies by Susanne et al., supporting the findings in our study. [13]
The mean microleakage values were lowest noticed in group IIB (0.9± 0.0.8) and the highest values were observed in group IA (2.8± 1.14). According to the findings of this current study, the microleakage detected in QTH light-cured samples is significantly higher than in samples cured by LED. Potentially this may be due to the coordination of LED optical output wavelength with the camphoroquinone absorption spectrum. LED light cure releases well-defined stimulated electrons. The output spectrum of LED is coordinated with the absorption spectrum of the camphoroquinone photoinitiator (450-500 nm). Therefore it does not need any filter. However, some studies indicate that the amount of dentinal microleakage in both LED light cure devices, and QTH is similar. It may be due to the different intensities of various applied light-curing units.[21], [22], [23], [24] The irradiance required for tetric Evo ceram bulk-fill (Ivoclar Vivadent) was about 70.2mW/cm2. For other bulk-fill resin-based composites the irradiance at a 4 mm depth was less than 10 perc of the irradiance on the surface. Nevertheless, at a 4mm depth DC was found to have scarcely decreased, suggesting initiator saturation.
Mills et al. stated that LED sources were capable of a significantly higher depth of curing for three different types of composite resins than were halogen LCUs. Oberholzer et al. reported substantially less microleakage at the dentine cementum interface when restorations were cured with an LED unit compared to curing with a standard halogen LCU.[25], [26] A natural consequence of light generation for the halogen lights results in the spectral distribution being very broad - from the deep infra-red (IR) to the hard ultra-violet (UV) region of the electromagnetic spectrum. So an extensive amount of heat is generated, which has to be filtered and discarded. The narrower spectral emission of the LED lights has an added advantage, as no light in the UV or IR range is generated, thus enabling these devices to be used without the types of filters which are needed in the QTH lights. Therefore, all the photons from the LED can participate in the curing reaction, and they can have sensitive wavelengths for the CQ initiator.[27], [28], [29] Within the limitation of the study, Incremental resin composite application alone is not enough to prevent or reduce the marginal microleakage. The polymerization shrinkage not only depends upon curing and placement techniques, but it also depends on the type of photoinitiator used.
Conclusion
When compared to the three experimental placement groups, the least microleakage was noticed in the incremental (IN) group, highest microleakage was seen in the bulk (BU) group. Among groups of light-curing sources, the least microleakage was seen in the LED group. With respect to subgroups, the least microleakage was observed in IN-LED (subgroup IIB), highest microleakage is seen in B-QTH (subgroup IA), interestingly there is no statistical difference between IN-QTH (sub group IIA) and CE-LED (sub group IIIB).
Conflict of Interest
The authors declare that they have no conflict of interest.
Source of Funding
None.
References
- QD Alomari, JW Reinhardt, DB Boyer. Effect of liners on cusp deflection and gap formation in composite restorations. Operative Dentistry 2001. [Google Scholar]
- G Bergenholtz, CF Cox, WJ Loesche, SA Syed. Bacterial leakage around dental restorations: its effect on the dental pulp. J Oral Pathol 1982. [Google Scholar] [Crossref]
- RS Agarwal, H Hiremath, J Agarwal, A Garg. Ashish Garg Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: An in vitro study. J Conserv Dent 2015. [Google Scholar] [Crossref]
- . . Gordon j chrestensen. clinicians report. serving dentistry 2012. [Google Scholar]
- EH Kim, KH Jung, SA Son, B Hur, YH Kwon, JK Park. Effect of resin thickness on the microhardness and optical properties of bulk-fill resin composites. Restor Dent Endod 2015. [Google Scholar]
- AR Yazici, C Celik, B Dayangac, G Ozgunaltay. Effects of Different Light Curing Units/Modes on the Microleakage of Flowable Composite Resins. Eur J Dent 2008. [Google Scholar]
- JG Leprince, WM Palin, J Vanacker, J Sabbagh, J Devaux, G Leloup. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent . [Google Scholar]
- AA Carvalho, FCL Moreira, LM Cunha, SM de Moura, JB de Souza, C Estrela. Marginal microleakage of class II composite resin restorations due to restorative techniques. Rev Odonto Ciênc 2010. [Google Scholar]
- K Hassan, S Khier. Composite resin restorations of large class II cavities using split-incremental horizontal placement technique. Gen Dent 2006. [Google Scholar]
- AA Alhabdan. Review of microleakage evaluation tools. J Int Oral Health 2017. [Google Scholar] [Crossref]
- MCP Nunes, EB Franco, JC Pereira. Marginal Microleakage: Critical Analysis of Methodology. Salusvitu Bauru 2005. [Google Scholar]
- V S Masamatti, VM Uppin. Evaluate the marginal microleakage in class ii composite restorations by four different placement techniques. Int J Dent Health Sci 2016. [Google Scholar]
- RR Nadig, A Bugalia, G Usha, J Karthick, B Vedhavathi. The effect of four different placement techniques on marginal microleakage in class II Composite restorations: An invitro study. World J Dent 2011. [Google Scholar]
- S Duarte, JRC Saad. Marginal adaptation of class II adhesive restorations. Quintessence Int 2008. [Google Scholar]
- V Chandrasekhar, L Rudhrapati, V Badami, M Tummala. Incremental techhniques in direct composite restoration. J Conserv Dent 2017. [Google Scholar]
- AH Tjan, BH Bergh, C Lidner. Effect of various incremental techniques on the marginal adaptation of class II composite resin restorations. J Prosthet Dent 1992. [Google Scholar]
- M Mubashir, M Baig, ZA Al Jeaidi, M Al-Muhaiza. Microleakage evaluation in restorations using different resin composite insertion techniques and liners in preparations with high c-factor - An in vitro study. King Saud Univ J Dent Sci 2013. [Google Scholar] [Crossref]
- LT Poskus, E Placido, PE Cardoso. Influence of placement techniques on Vickers and Knoop hardness of class II composite resin restorations. Dent Mater 2004. [Google Scholar]
- S Duarte, W Dinelli, MH Da Silva. Influence of resin composite insertion technique in preparations with a high C-factor. Quintessence Int 2007. [Google Scholar]
- S Szep, H Frank. Comparative study of composite resin placement centripetal buildup versus incremental technique. J Pract Esthet Dent 2001. [Google Scholar]
- F Zakavi, LG Hagh, S Sadeghian, V Freckelton, A Daraeighadikolaei, E Ghanatir. Evaluation of microleakage of class II dental composite resin restorations cured with LED or QTH dental curing light; Blind, Cluster Randomized, In vitro cross sectional study. BMC Res 2014. [Google Scholar] [Crossref]
- GJ Fleming, S Khan, O Afzal, WM Palin, FJ Burke. Investigation of polymerization shrinkage strain,associated cuspal movement and microleakage of MOD cavities restored incrementally with resin-based composite using an LED light curing unit. J Dent 2007. [Google Scholar] [Crossref]
- RS Queiroz, MC Bandeca, LR Calixto, EG Saade, MR Nadalin, MF Andrade. Effects of light curing units on microleakage under dental composite resins. Laser Phys 2009. [Google Scholar] [Crossref]
- MR Bouschlicher, FA Rueggeberg, DB Boyer. Effect of stepped light intensity on polymerization force and conversion in a photo activated composite. J Esthet Dent 2000. [Google Scholar] [Crossref]
- F Yilmaz. Effects of different light sources on microleakage of composite resins with different monomer structures. J Dent Sci 2013. [Google Scholar] [Crossref]
- T G Oberholzer, IC Du Preez, M Kidd. Effect of LED curing on the microleakage, shear bond strength and surface hardness of a resin-based composite restoration. Biomaterials 2005. [Google Scholar] [Crossref]
- AM Chandurkar, SS Metgud, SS Yakub, VJ Kalburge, BC Biradar. comparative evaluation of the effects of light intensities and curing cycles of QTH, and LED lights on microleakage of class v composite restorations. J Clin Diagn Res 2014. [Google Scholar]
- N Krämer, U Lohbauer, F García-Godoy, R Frankenberger. Light curing of resin-based composites in the LED era. Am J Dent 2008. [Google Scholar]
- PD Hammesfahr, MT Connor, X Wang. Light-curing technology: past, present, and future. Compend Contin Educ Dent 2002. [Google Scholar]