- Visibility 189 Views
- Downloads 12 Downloads
- DOI 10.18231/j.idjsr.2022.006
-
CrossMark

Mucocele of lower lip – Case reports
Introduction
Mucocele is a mucous filled cyst that appear in the oral cavity. It is a painless, asymptomatic, soft tissue benign lesion and non-infective salivary gland swellings of oral cavity. The term mucocele is derived from Latin word where “muco” means mucous and “cele” means cavity. Mucocele is the most common salivary gland lesion in the oral cavity. They are most commonly found on the lower lip, lateral to the midline.[1] They are rarely seen on the upper lip, retro molar pad or palate. They may occur at any age, but are seen most frequently in the second and third decade of life. These lesions have no sex predilection. Mucocele of the oral mucosa results from an alteration of minor salivary glands due to a mucous accumulation causing limited swelling. [2] Two types of mucocele can appear - extravasation and retention. Extravasation mucocele results from trauma to salivary glands duct and the consequent spillage into the soft tissues around this gland. Retention mucocele appears due to a decrease or absence of glandular secretion produced by blockage of the salivary gland ducts. Mucoceles present a bluish, soft and transparent cystic swelling. The blue colour is caused by vascular congestion, and cyanosis of the tissue above and the accumulation of fluid below the mucosa. [3]
Case Report 1
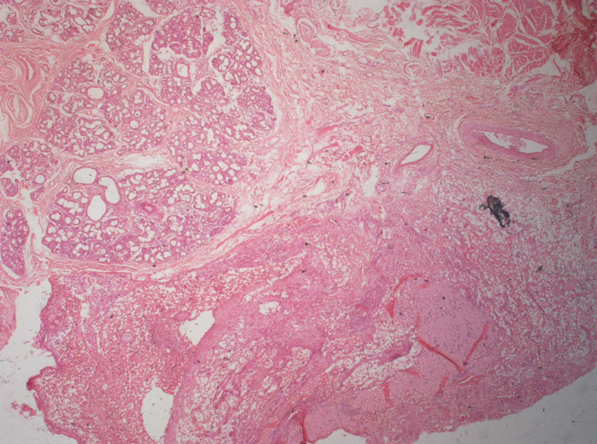
A 12-year old boy patient reported with the chief complaint of painless swelling of lower lip since 2 months. Patient had a history of reduction in the size of swelling one month back and which again increased in size. On examination a solitary swelling was present on left side of lower lip about 1x0.5 cm in size, oval in shape, have ill-defined borders, mucosa over it appears pink in colour, soft in consistency, fluctuant, non-tender. Based on history and clinical examination provisional diagnosis of mucocele of lower lip was given. Routine hematologic investigations were carried out before excisional biopsy. The excised specimen was sent for histopathologic examination. Histopathology report revealed mucous pool which is surrounded by granulation tissue. The granulation tissue may consists of inflammatory cell infiltrate, collagen fibres, blood vessel and the connective tissue stroma contains salivary gland acini. The submucosal shows presence of muscle fibres, adipocytes suggestive of mucocele of lower lip. After excision regular recall and checkup for the reoccurrence of the lesion was done for 6 months.
Case Report 2
A 7 year old boy patient came with the chief complaint of painless swelling of lower lip since 1 months. Patient had lip biting habit. Patient had a history of recurrent appearance of swelling of lower lip. On examination a solitary swelling present on left side of lower lip about 1x0.5 cm in size, oval in shape, have ill-defined borders, mucosa over it appears pink and white in colour, soft in consistency, fluctuant, non tender. On intraoral examination mixed dentition was present and root stump present irt 74. Based on history and clinical examination provisional diagnosis of mucocele was given. Routine hematologic investigations were carried out before excisional biopsy.



Discussion
Mucocele is a mucous filled cyst that appear in the oral cavity. It is a painless, asymptomatic, soft tissue benign lesion and non-infective salivary gland swellings of oral cavity. The term mucocele is derived from Latin word (muco - mucous and cele – cavity). Mucocele is the most common salivary gland non-neoplastic lesion in the oral cavity. Mucocele of the oral mucosa results from an alteration of minor salivary glands due to a mucous accumulation causing limited swelling. [4]
Two types of mucocele can appear -
Extravasation type
Retention type. [4]
Extravasation mucocele results from trauma to salivary glands duct and the consequent spillage into the soft tissues around this gland. Retention mucocele appears due to a decrease or absence of glandular secretion produced by blockage of the salivary gland ducts. In children extravastion type is most common.
Etiology
Yamasoba et al [5] has highlighted two crucial etiological factors for occurrence of mucocele:
Trauma to salivary gland.
Obstruction of salivary gland duct.
Pathogenesis
Extravasation mucocele results from broken salivary gland duct causing spillage into the soft tissues around the gland. Extravasation mucoceles undergo three evolutionary phases. In the first phase, mucous spills from the excretory duct into surrounding tissues where some leukocytes and histiocytes are found. In second phase granulomas become visible during the resorption phase due to histiocytes, macrophages and multi-nucleated giant cells associated with a foreign body reaction. In the final phase, connective cells form a pseudo capsule without epithelium around the mucosa. [6], [4], [7]
Retention mucoceles are formed by dilation of the duct secondary to its obstruction caused by a sialolith or dense mucosa. The majority of retention cysts develop in the ducts of the major salivary glands. [6], [4]
Clinical presentation
Clinical appearance of both extravastion and retention type mucoceles is similar. Incidence of mucocele in general population is 0.4 – 0.9 %. Most common in 1st – 2nd decade of life. There is no sex predilection. [8]
Location: Extravasation mucoceles appear frequently on the lower lip lateral to midline(53%) followed by buccal mucosa-4%, floor of mouth-5%, ventral surface of tongue-1%, palate -1%, upper lip 2% [9] and are rarely found in the retromolar region, soft palate and posterior dorsal area of tongue; in contrast, retention mucoceles appear at any site in the oral cavity. Majority of mucoceles occurred in the lateral part of the lower lip which is the more trauma prone site. This finding supports the role of chronic trauma as an etiologic factor either in the form of sharp tooth cusp, or proclined anterior teeth or biting habit for the formation of mucoceles. [1] Mucoceles arising on the ventral surface of the tongue are known as mucocele of the glands of Blandin-Nuhn. These glands are located near the ventral tip of the tongue and are arranged in a mass with a horseshoe shape. They are embedded in the muscles of the ventral aspect near the midline. Mucoceles of the glands of Blandin-Nuhn are considered to be rare. [10] When located on the floor of the mouth, these lesions are called ranulas because the inflammation resembles the belly of a frog. [4]
Mucoceles appear as asymptomatic pedunculated or sessile swelling or as fluid filled vesicle or blister in the superficial mucosa or as a fluctuant nodule deep within the connective tissue. But they may causes discomfort, interferes in speech and mastication.
Mucoceles present as bluish, soft, and transparent cystic swelling that frequently resolve spontaneously. Blue color is due to vascular congestion, cyanosis of the tissue above, and accumulation of fluid below. Colour may vary depending on the size of the lesion, proximity to the surface and elasticity of overlying tissue. Sometimes due to constant friction or trauma the lesion surface may appear whitish in color due to keratinization. These mucoceles are more commonly round to oval in shape having ill-defined borders. These swelling appears soft to rubbery in consistency. [4], [11], [8], [1], [12], [7] These mucoceles are fluctuant and they may rupture following trauma and reappear after epithelium heals. Traumatic neuroma, Traumatic fibroma, Lipoma, Haemangioma, Varix, Tumors of minor salivary gland, Lymphangioma are considered as differential diagnosis for mucocele of lip.
Diagnosis of mucocele can be done by taking proper case history, positive history for lip biting or sucking habit, trauma, rupture and reappearance of swelling, varying in size. Radiographic evaluation is needed to rule out if sialoliths are considered a contributing factor in the formation of oral and cervical ranulas. The fine needle aspiration cytology demonstrates the mucus retention phenomenon. The chemical analysis could disclose protein content and high amylase. The localization, determination of the origin of the lesion, visualize the form, diameter, position of lesion relative to adjacent organs can be done by computed tomography scanning and magnetic resonance imaging especially incase of ranula. [13] Histopathology in the case of retention mucoceles a cyst cavity can be found, this is generally well defined with an epithelial wall covered with a row of cuboidal or flat cells produced from the excretory duct of the salivary glands . Compared to extravasation mucoceles, retention mucoceles show no inflammatory reaction and are true cysts with an epithelial covering. Extravasation mucoceles are pseudocysts without defined walls. The extravasated mucous is surrounded by a layer of inflammatory cells and then by a reactive granulation tissue made up of fibroblasts caused by an immune reaction. Even though there is no epithelial covering around the mucosa, this is well encapsulated by the granulation tissue. [4], [14], [3] Treatment modalities include conservative surgery, marsupilization, micro-marsupilization, carbon-di-oxide laser ablation, intra-lesional injection, gamma linolenic acid and cryosurgery. Out of many advanced treatment modalities simple surgical excision with care is the treatment of choice. Surgical excision with removal of the involved accessory salivary gland has been suggested as the treatment. Reoccurrence can be avoided by removing adjacent surrounding glandular acini and removing the lesion down to the muscle layer. Special care should be taken to avoid injury to adjacent glands and ducts while placing sutures as this also causes reappearance. [15]
Conclusion
Mucoceles are one of the most common soft tissue lesions of the oral cavity which causes distress and discomfort to patient. It is Dentists who usually come across these lesions when patients comes for a routine oral check or an dental problem. Management of mucocele becomes challenging due to high recurrence rate. However, surgical excision with dissecting surrounding and contributing minor salivary gland acini proved to be successful with least recurrence.
Conflict of Interest
The authors declare that there is no conflict of interest.
Source of Funding
None.
References
- M S Greenberg, M Glick, J A Ship. Burket’s Oral Medicine. 11th edn.. 2008. [Google Scholar]
- JV Bagán Sebastián, FJ Silvestre Donat, MP Diago, MA Milián Masanet, P Diago. Clinico-pathological study of oral mucoceles. Av Odontoestomatol 1990. [Google Scholar]
- C B More, K Bhavsar, S Varma, M Tailor. Oral mucocele: a clinical and histopathological study. J Oral Maxillofac Pathol 2014. [Google Scholar] [Crossref]
- J Ata-Ali, C Carrillo, C Bonet, J Balaguer, M Peñarrocha, Peñarrocha. Oral mucocele: review of the literature. J Clin Exp Dent 2010. [Google Scholar]
- T Yamasoba, N Tayama, M Syoji, M Fukuta. Clinicostatistical study of lower lip mucoceles. Head Neck 1990. [Google Scholar]
- N Bhargava, M Sidiq, P Agarwal, P Narain. An Unusual Presentation of Oral Mucocele in Infant and Its Review. Case Rep Dent 2014. [Google Scholar] [Crossref]
- L Bodner, E Manor, BZ Joshua. Oral Mucoceles in Children--Analysis of 56 New Cases. Pediatr Dermatol 2015. [Google Scholar] [Crossref]
- S Laller, RS Saini, M Malik, R Jain. An Appraisal of Oral Mucous Extravasation cyst case with Mini Review. J Adv Med Dent Sci Res 2014. [Google Scholar]
- D Re Cecconi, A Achilli, M Tarozzi, G Lodi, F Demarosi, A Sardella. Mucoceles of the oral cavity: a large case series (1994-2008) and a literature review. 2010. [Google Scholar] [Crossref]
- Y Jimbu, M Kusama, H Itoh. Mucocele of the glands of Blandin-Nuhn: clinical and histopathologic analysis of 26 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003. [Google Scholar] [Crossref]
- P Chaitanya, D Praveen, M Reddy. Mucocele on Lower Lip: A Case Series. Indian Dermatol Online J 2017. [Google Scholar]
- NB Nagaveni, M Bajaj, S Pathak, AS Shruthi, P Poornima. Mucoceles of the oral cavity in Indian pediatric patients: A retrospective study. Int Dent Med J Adv Res 2015. [Google Scholar] [Crossref]
- KU Nallasivam, BR Sudha. Oral mucocele: Review of literature and a case report. J Pharm Bioallied Sci 2015. [Google Scholar] [Crossref]
- R Rajendran. Shafer's textbook of oral pathology. 7th . 2009. [Google Scholar]
- N Singh, P Chandra, S Agarwal. Oral mucocele: A case report. J Dentofac Sci 2014. [Google Scholar]