Introduction
Oral carcinomas are the fifth most common carcinoma worldwide.1 The course of the disease and its management has a huge effect on psychological and functional wellbeing of the patient.2 Oral cancer management involves many treatment modalities like surgery, radiotherapy and chemotherapy etc. Besides the elimination of the carcinoma, regaining the patient’s aesthetics and oral function which was lost or altered is also of prime importance.
Primary oncology surgery can impede prosthodontic rehabilitative goals. These effects include an altered oral anatomy, compromised soft tissue conditions like missing or scarred tissues, bulky flaps, altered muscle attachments, restricted mouth opening, loss of lip competence, loss of hard tissue such as bone or teeth and alternations in facial profile.3 Rehabilitating such oral defects remains a challenge because of the limitations in management options, commonly due to lack of support or space for the prosthesis, impeded resiliency of soft tissues and loss of integrity. Studies that have looked into the quality of life of patients post oral cancer surgeries has reported that prosthodontic rehabilitation of lost oral function is of at most importance. 4, 5
Among the several prosthodontic measures in rehabilitating an oral cancer treated patient, an obturator prosthesis remains widely used by the maxillofacial prosthodontists and well accepted by the patients. This clinical case report describes in detail of patient affected by carcinoma of left hard palate post primary surgery and pre radiotherapy treatment modalities.
Case Report
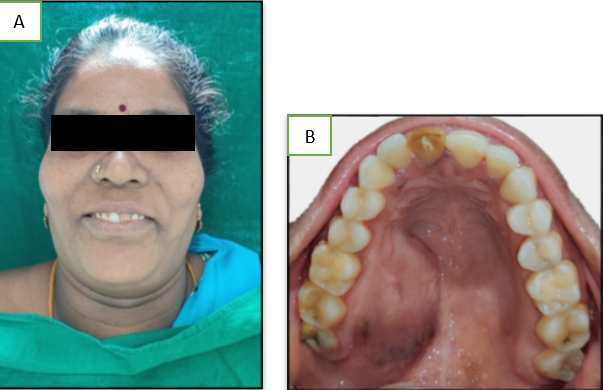
A 38 year old female patient reported to the department of maxillofacial surgery with the chief complaint of swelling in the palatal region. (Figure 1 a) On intraoral examination she presented with a swelling in the left hard palate confined to the posterior maxillary region. (Figure 1b) A discoloured tooth - #21 was also present. Oral hygiene was satisfactory on examination.



















Clinical and radiographical examination was carried out. On histopathological examination, carcinoma of palate was diagnosed and the clinical findings were confirmed. The patient was then referred to the post graduate clinics of department of maxillofacial prosthodontics for construction of a surgical obturator / plate.
The pre operative impression was made using irreversible hydrocolloid (Hydrogum 5, Zhermack, Italy) in a perforated dentulous tray. (Figure 2) The impression was poured with dental stone (Gyproc, Prevest Denpro, Jammu, India) to produce the positive template/cast. The area for resection was marked and sent by the surgeon and immediate surgical obturator was fabricated accordingly. (Figure 3)
In the operating room resection of left maxilla was done to remove the tumor and a surgical closure was attempted using the adjacent soft tissues. The surgical obturator was inserted immediately after resection of the left maxilla and held in position using C-clasps on the remaining natural teeth thereby, providing the tripod stabilization for the obturator prosthesis. (Figure 4) One week after surgery the patient was reviewed to rule out complications and proper position of the plate was ensured. The patient presented with a maxillectomy defect extending from the midline to the soft palate in the left side. (Figure 5)
Clinical intra-oral examination showed a hollow remaining with an oro-nasal communication, while the remaining teeth, gingiva and other half of the palate appeared within the normal limits. Lack of oral hygiene may have been due to limited mouth opening and plate in her oral cavity. Extra-oral examination showed a curved profile, an asymmetrical face, no deviation of mandible, no palpable or tender lymph nodes and normal TMJ in function. The defect is under Aramany class I classification. The patient was instructed on removal and repositioning the plate and maintenance a good oral hygiene.
A month later, patient reviewed clinically, intra- and extra- oral examination revealed a good initial healing at the defect site and sutures were evident. The surgical plate was modified by molding the anterior and posterior border seal using green stick compound (HiFlex, Prevest Denpro, Jammu, India) and a pick-up impression using irreversible hydrocolloid material ((Hydrogum 5, Zhermack, Italy) in a perforated sectional stock tray. (Figure 6a) Beading and boxing of impression was done with modelling wax (Hindustan Modelling wax no:2, India). (Figure 6b) The impression was poured with dental stone (Gyproc, Prevest Denpro, Jammu, India) to produce the positive template/cast. Auto-polymerizing resin was added to seal the borders in the old surgical plate. The modified surgical plate was finished, polished and inserted into the patient’s mouth. (Figure 7a & b)
Patient reviewed after 3 weeks prior radiotherapy, the clinical intra- and extra-oral examination was done and healing status of the defect site was re-assured. (Figure 8) The fabrication of an interim obturator was initialized. Maxillary and mandibular impressions were made using irreversible hydrocolloid material (Hydrogum 5, Zhermack, Italy) in a perforated dentulous tray. (Figure 9a) The impression was poured with dental stone (Gyproc, Prevest Denpro, Jammu, India) to produce the positive template/cast and wax spacer was adapted on the remaining natural teeth of the cast for custom tray fabrication (Figure 9b)
A custom tray using auto-polymerising resin (DPI RR Cold Cure Repair Material Powder, India) was fabricated with loop (21 gauge stainless wire) secured in the tray with auto-polymerizing resin. (Figure 10) Border molding was done to seal the defect area confined to the left maxillary palatal region using green stick compound. (Figure 11) The intra oral defect was recorded by engaging green stick compound to the wire loop and the other parts of the custom tray (Figure 12) A wash impression was made in putty and monophase polyvinyl silicone impression material (Aquasil Lv ultra, smart wetting impression, Dentsply, Detrey Gmbh, Germany). (Figure 13)
The beading and boxing of final impression was done.(Figure 14). The impression was poured with dental stone (Gyproc, Prevest Denpro, Jammu, India) to produce the positive template/cast. (Figure 15) The usual steps in fabricating the conventional acrylic partial denture were followed. (Figure 16, Figure 17, Figure 18, Figure 19) The retention for this type obturator was gained from the remaining teeth with wrought wire clasps on teeth 11, 14, 16. The processed interim obturator was inserted (Figure 20). Patient was reviewed for retention and patient comfort after one week, on intra oral examination, the defect site revealed no pathologies due to the prosthesis. (Figure 20) A follow up system will be scheduled three months later, post-radiotherapy and the soft tissue status will be evaluated.
Discussion
Rehabilitation of patients with acquired maxillary defects is relatively simpler than rehabilitation of defects in the mandible and pleasing as well as accepted outcomes can be identified at the end of the treatment. On the other hand, great efforts should be given in dealing with large defects to obtain the substantial requirements for retention and support of the prosthesis. 6 The infiltrative nature and pattern of squamous cell carcinoma in oral cavity makes it difficult to remove completely, which explains its high recurrence rate and need for radiotherapy.
Prosthodontic rehabilitation of maxillary acquired defects could be organized into three stages of treatment. For each step a different type of obturator is fabricated. 6
Immediate Surgical Obturator/ Plate
This type of obturator is fabricated from an impression obtained prior to the surgery day and inserted post resection of the tumor. Advantages of using surgical obturator include- 1. Can form a barrier between the oral cavity and wound during the initial healing phase and 2. It enables the patient to speak and swallow more effectively. 6, 7
Interim Obturator
Three to four weeks after resection, the construction of interim obturator can be started.8 This type of obturator is totally acrylic incorporated with wrought wire clasps engaging the remaining natural teeth for retention. Patient should be reviewed every two weeks as the healing progresses and lining materials can be placed. In this case, fabrication of interim obturator was performed after 4 weeks of surgery. Retention was gained from the remaining natural teeth by incorporating wrought wire clasps.
Definitive Obturator
Defective obturator should not be constructed unless there is complete healing of the defect site and it is dimensionally stable. It may take up-to 3 to 6 months varying according to many factors.9 For this case, a definitive obturator will be scheduled after reviewing the healing status of the defect post radiotherapy.
Quality of life of patients with maxillary defects can be improved by a properly designed obturator prosthesis. These types of obturator can restore mastication, swallowing, esthetics, resonance and speech.
Conclusion
A proper diagnosis and a well designed treatment plan will produce desirable outcomes. Rehabilitation with obturator prosthesis always remains to be a functional and effective treatment modality. This paper discussed the prosthetic management of acquired maxillary defect prior to radiotherapy using an obturator prosthesis.
Informed Consent
The authors certify that the patient has given her consent for use of her images and other clinical information to be used in the journal. The patient is also informed and understands that her name and initials will not be published and due efforts will be taken to conceal her identity.