Introduction
SARS-CoV-2 assessed to be originated from Wuhan, China, has massively affected the world in the year 2020, bringing most facets of public life to a standstill.1 It has a major detrimental effect because of it high virulence and unpredictable mutation forms, causing shutdown of businesses, crowded hospitals and a strain on the health sector, as well as causing the cessation of operation of educational institutions.2 Maintaining distance from people who were not household members was advised. Almost every non-essential worker encouraged to stay in their home, which forced them to have to adapt their way of life to working from home. Those who did not have the means to work or study from home suffered heavily.3
Like other institutions, educational institutes of all kinds were affected. They were ordered to shut down, as even though young people were not as susceptible to symptomatic COVID-19, they still posed the risk of unknowingly transmitting SARS-CoV-2 to more vulnerable members of the community.4 Keeping nearly 500 million students at home for an undetermined period of time was harmful to their future, putting their educational progress in jeopardy. They needed to be provided a structure and incentive to continue their learning with as little disruption as possible.5
To counter this problem, many educational institutes took the aid of online conference platforms like Zoom®, Google Classroom®, or Microsoft Teams® to carry out their curriculum as usual, which worked for most aspects.6 Major problems were faced by the students in medical education, which is still struggling to adapt the demanding curriculum to online teaching mediums. Not only does medical education rely on large bundles of theoretical data but also implements much practical experience to better teach their respective medical or dental students.7
Of the medical students, dental students, especially those in their clinical years, spend much of their learning time either in simulation labs practicing on models, or interacting with patients at different levels of supervision.8 Manual dexterity with consistent practice and supervision is an essential part of dental educational programs, and it cannot be left out due to the current pandemic for clinical students or those in post graduate programs. Some dental schools with in well-resourced countries have the necessary funding and infrastructure to introduce students to clinical skills in simulation labs with cubicles without violating any standard operating practices.9
However most dental schools, particularly in less prosperous countries, struggle with this aspect as they do not have the finances for either virtual model training, nor simulation labs large enough with COVID-19-safe partitions in place. Ordinarily they rely heavily on direct observation, assistance, and supervised procedures on live patients.10 Furthermore, online education is a new phenomenon in the educational sector in many countries, and most students and teachers are coming to terms with how to integrate it adequately in their programs. Internet connection and lack of enough technical hardware for online classes are also major problems anticipated in these countries for online education.11
Uninterrupted education is a major necessity even amongst the COVID-19 pandemic and the adaptation to online delivery is a welcome initiative. However, it also needs to be consistently improved and adapted to the needs and expectations of the students using it. This study aims to assess the perception of dental students in Pakistan, Egypt, and India of their online classes, and their input on what improvements they recommend, considering their own curriculum needs.
Materials and Methods
The study was approved by the board of ethics, Gandhara University Peshawar, Pakistan. This was a cross-sectional online survey in which self-administered questionnaires were distributed through different social media platforms. Completed questionnaires were automatically uploaded to Google spreadsheet software. The target population was all dental students, both undergraduate and postgraduate, residing in 3 countries with similar level of infrastructure: Pakistan, Egypt, and India. The name and institution of participants was anonymized to protect their privacy. The sampling technique performed was convenience sampling.
The questionnaire
A structured, self-administered questionnaire aimed to assess the perception of dental students of online dental education now that it was their only mode of education. After composition, the survey questionnaire was assessed separately by two delegates from the Peshawar Department of Dental Education, where they ranked questions on a relevance scale. The investigators revised the questionnaire accordingly. To reduce response biases such as social desirability bias, participants were informed of their demographic information staying anonymous. After filling out their consent to participate in the survey, their demographic information was collected, with the questions following. The first set of questions focused on whether the students had access to appropriate devices, knowledge and internet connectivity sufficient to take their online dental classes with ease.
The second part of the questionnaire assessed the comfort and convenience of the students with taking online classes from home, their concentration and uptake of knowledge during class, and whether they felt their teachers had the right training to ensure seamless interaction between them and the students. Other questions assessed whether the students preferred the learning experience of online or multimedia education regarding clinical subjects, or hands-on demonstrations in the ward.
Then the questions turned to their opinion regarding the effect of the surge in webinars on dental education, as well as dental community reaching out through their social media platforms was for their learning experience, and their opinion on dental conferences going virtual.
The last part of the questionnaire was open-ended which directly asked the students input on their experience of online dental classes, and improvements they would like in the medium of online learning.
Results
A total of 565 responses were collected out of which 67 were rejected due to incomplete submissions and duplicated results, for an N of 498. The mean age of the population was 22.3 years, with a standard deviation of 4. The demographic characteristics are given in the table below.
Table 0
Overall, almost 30% (146) of the population stated that they did not have an internet connection suitable to run online lecture delivery applications and experienced lag and disconnection. In terms of learning experience 34% (173) found online lectures were not helpful for their dental education. More than half the population (51%, 257) lacked concentration during their online lectures. Also, 60% (299) of the participants felt that the teachers were incapable of giving attention to individual students during the online classes. A very large number of participants (71%, 358) expressed that their teachers required more training on how to deliver lectures adequately through online teaching platforms. All of these answers were statistically significant with a Chi-square test score of 0.001.
Students of clinical years further expressed that they lacked a proper understanding of their clinical subjects at 76% (379). This too was statistically significant with a chi-square test score of 0.003.
Discussion
The COVID-19 pandemic brought the process of conventional education to a standstill, and also revealed how underprepared the world was in terms of adapting to this issue despite many months of warning. This research aimed to assess dental students’ perception of the quality of their online education delivered during the quarantine period of the COVID-19 pandemic in three countries with similar infrastructure for teaching: Egypt, India, and Pakistan.
Good quality internet connections are still a luxury in these countries. A recent study of internet in Pakistan, found that 42% of dental students there had connectivity issues.12 In this study, almost 30% (p=0.001) did not have the adequate internet capacity for seamless online classes. This was in contrast to a study done in Germany citing more than 95% having stable internet connection.13 There was a significant gap in communication between the students and teachers during online learning, where almost 60% felt that the teachers needed more training on how to use online teaching platforms, which was again in contrast to countries with more positive responses from both the students and teachers like Germany.13
Although online education had become a necessity for the duration of the lockdown, it did receive some negative reviews where 34% expressed that online education was not quite helpful for their dental education, which was similar to what dental students in central India voiced, where 25% did not find them useful while another 24% were not sure about it. Saudi Arabia it stood even higher at 70% dissatisfaction with online learning for dental sciences.14 The same can be said about Nepal, where more than 85% of the teaching faculty were not warm towards online classes.15 More than half the population (57%) said that they would prefer a live lecture rather than a recorded one, in terms of having better interaction with the teacher. This stood in contrast to India where, almost 72% preferred online medium of education, however they did not specify the exact reason for it.16
In the era of social media, concentration deficit has become a pandemic of its own. This can be further exacerbated during online classes where students can freely browse their social application or other forms of entertainment during their lectures.17 More than half of the participants in our study admitted to a lack of concentration during an online lectures. This was coupled by 60% of the students having reservations that their teacher does not impart the same level of attention to individual students and more than 70% felt that they needed more training on how to teach through online platforms. Countries with a higher level of infrastructure marked a clear difference here as study displayed that even though 60% of the teaching staff was not familiar with online learning platforms, they adapted very quickly and the students had a higher satisfaction score from their dental faculty.13
One of the most important aspects of a dental undergraduate program is the development of clinical skills which will enable graduates to adeptly carry out routine procedures with ease. This aspect seemed to suffer the most, as more than 58% of the participants were of the opinion that online education is more suited for basic sciences than clinical dental sciences, 76% regarding their knowledge of clinical subjects as unsatisfactory, and almost 65% were of the opinion that the way to develop clinical skills was to practice them on mannequins or on patients under supervision. The countries with more educational resources fared far better as they resumed their clinical training by using smaller groups to go for clinical practice on mannequins.13, 18 Unfortunately these type of facilities still cannot be afforded by most dental institutes in much of the world.
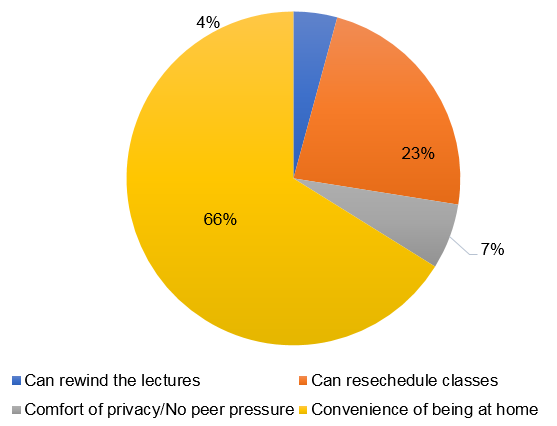
There were many perceived benefits from the current mode of online learning as a majority of participants agreed that having to attend classes at home has been very convenient for them. They did not have to go through the daily commute, and saved hostel charges and other expenses. More than half the participants also agreed that their learning experience was much better from the comfort of their homes behind a virtual barrier. The type of personality of the student also affects their preferred mode of education as demonstrated by another study. 19
Over the course of the pandemic, many of the esteemed dental educators of the world took to online platforms, as a means to continue sharing their experience and knowledge with the rest of the community which received generally positive reviews. However, during that same time majority of the undergraduate students questioned the price of that online curriculum, even though they deemed it important for their education.
Limitations
The perceived limitation of the study can be that we could not achieve an equal number of students from our target countries which imbalanced our results.
Conclusions
Online education became a necessity during the COVID-19 pandemic; however, it did not receive positive reviews from dental students in countries with under-developed educational and internet infrastructure. Students lacked both motivation and concentration while participating in online learning, and more than half thought their dental educators needed more training in providing a seamlessly interactive learning experience. In both the close ended and opinion section students agreed that their teachers could not focus on individual students and needed more training.
The most profound advantage for most students was the convenience of being at home and being able to reschedule lectures if not feasible.
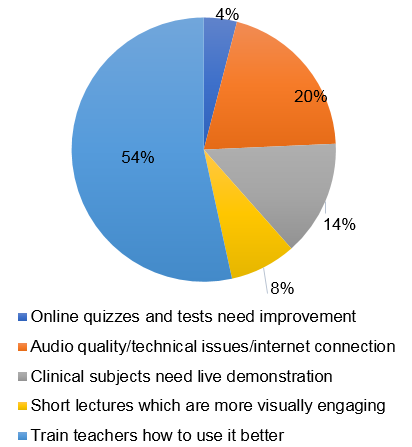
Network problems was one of the major issues faced by some dental students. Basic sciences could be taught well using online platforms, however more than half the students felt that their clinical skills were lagging due to no practical demonstrations and supervised training, and online classes were more suited for basic rather than clinical classes. More than 30% felt that online classes were not helpful at all for their dental education. Most institutes should revise their curriculum for clinical dentistry to adapt it better to the current scenarios.