Introduction
Piercing is a worldwide form of body art and has become increasingly popular in western society.1 Piercing refers to the infiltration of the jewellery into the body areas such as the eyebrows, ears, tongue, nose, lips, navel and genitals. Oral and perioral piercing has been practiced for a long time for various religious, cultural, sexual or identical reasons and has been believed and practiced autonomously all over the world.2 With today's fast-growing generation, a desire for distinctive identity is the main factor responsible for such piercings.1, 2 Lately oral piercings has gained popularity among teens and young adults. Self-representation in these age groups has increased significantly and they go towards extreme to get desired results. Other contributing factors are daring behaviour, independence of spirit and enhancing the body as per the fashion.3, 4 In oral cavity tongue piercing is the most common, followed by lips. Piercing has entered a new sphere involving other areas such as frennum, uvula, philtrum, cheeks and even tongue splitting. Frequently used jewelry for such piercings are barbell, studs, labret, captive beads, rings etc.1, 2, 3, 4, 5
Even though individuals succeed in expressing themselves, but many of them are unaware of the associated risks. It is important to know that oral and perioral piercings not only affect oral health, but also cause other long-term systemic damage if not treated with care.6 Many local and systemic complications have been observed as a consequence of oral and perioral piercing which include;
Immediate complication
Edema of the tongue leading to airway obstruction, pain of tongue affects speech, mastication and deglutition. 7, 8
Anaphylactic reactions can be caused by some of the materials e.g., nickel. 9, 10
Hyper salivation, puncturing the tissues without proper measures can cause severe hemorrhage
Trigeminal nerve damage: inferior alveolar and superior alveolar are commonly involved, lingual nerve damage usually seen in tongue piercings.8,9,10
Aspiration of jewelry during the uvula piercing or tongue piercing, can lead to choking and death of the patient. 11
Delayed complication
Ulcerations
Plaque accumulation can produce halitosis and possible infections.12
Endocarditis is the most common and potentially due to Neisseria mucosa and Haemophilus aphrophilus. 13, 14, 15
Trauma to lingual gingiva, erythema and edema of gingiva due to rubbing the ball in the lingual gingiva.16
Periodontal attachment loss involving proximal teeth. 16, 17, 18
Ludwig’s angina usually due to frenulum and lingual piercing. 19
Fracture of the tooth occur by biting the barbell, careless jewelry insertion, talking, eating etc. 24, 25, 26
If tongue piercing goes wrong, bifid tongue can be a serious complication. 27
Gingival recession due to continuous friction of the gingiva with the jewellery. 28, 29
Pulpal sensitivity from contact between galvanic currents in stainless steel ornaments and other intra-oral jewellery.9, 19
Radiopacity of piercing jewelry is seen during X-ray examinations. Hence for panoramic X-.rays, removing metal objects above the neck is a must. 11
Most dangerous oral site for piercing is the uvula, due to the increased chances of airway obstruction. It has been found that piercing is a potential route for the transmission of viruses such HIV, hepatitis (B, C, D and G), herpes simplex and Epstein-Barr. 30
They have mentioned congenital deformities and the possibility of cerebellar abscesses. 31
As dental students, it is the responsibility of each and every student to educate their peer groups as well as the patients about the effect of piercing and how it acts as a double edge sword.
Materials and Methods
The present study is a questionnaire based survey on the awareness of complications related to oral and perioral piercing which was conducted online using Google forms. In total 145 undergraduate students of a private dental college haryana participated in this survey. A total of 10 questions were asked from the participants. The participants replied to the survey by clicking appropriate options. The questionnaire was self- conceptualized and its authenticity was made by discussing it with faculty of the department of Oral Medicine and Radiology. The survey was approved by institutional ethical committee. After the data collection, it was compiled and presented in the form of pie charts and bar diagrams.
Results
A total of 145 subjects participated in the study and the data was evaluated with pie charts and bar diagrams.
Figure 1
Have you ever heard of or seen oral and perioral piercing?88.2% have heard or seen oral and perioral piercing, 9% have never seen or heard of oral and perioral piercing and 2.8% responded with maybe.
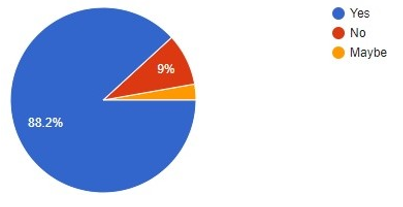
Figure 2
If yes then from where?
83.6% said they saw it in movies 38.1% read it in articles 37.3% heard it from friends and 4.5% from family members.
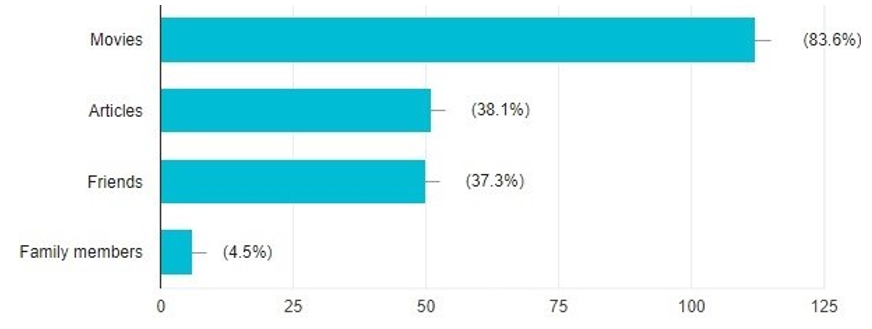
Figure 3
What is the most common site?
51.4% responded with most common site as tongue 30.3% said lower lip 9.9% said upper lip 8.5% responded as philtrum.
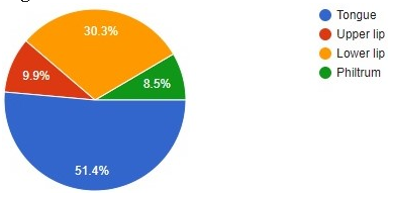
Figure 4
Click on the options you think are the piercing sites.
As far as the knowledge of other piercing sites are concerned only 6.4% knew that uvula is also pierced 19.3% knew about cheek 22.9% knew about frennum 88.6% about lips and 87.1% about tongue.
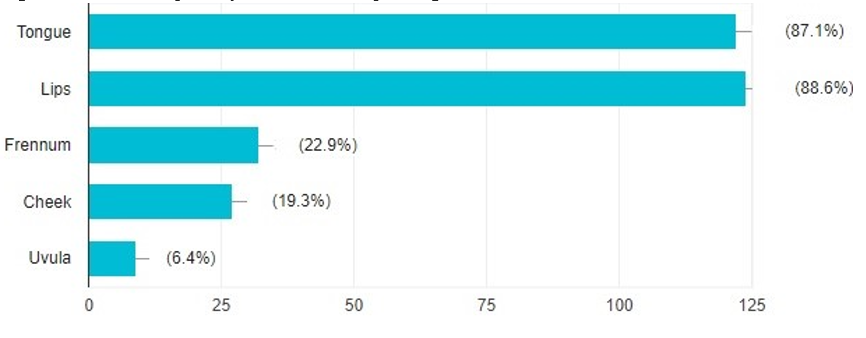
Figure 5
Do you think there occurs any complications after oral and perioral piercing is done?
While enquiring about the complication, 71.6% responded as yes that there exist complications related oral and perioral piercing 25.5% responded as maybe and 2.8% didn’t know about the complications.
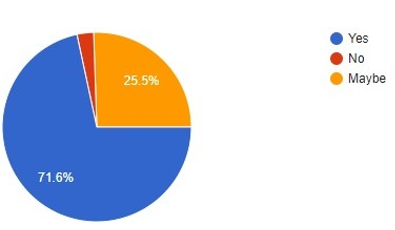
Figure 6
What according to you are the complications of oral and perioral piercing?
88.9% knew ulceration as a complication 62.2% knew about edema and hemorrhage. 35.6% had a knowledge about gingival recession 30.4% were aware of hepatitis 22.2% knew about endocarditis and only 18.5% were familiar about Ludwig’s angina.
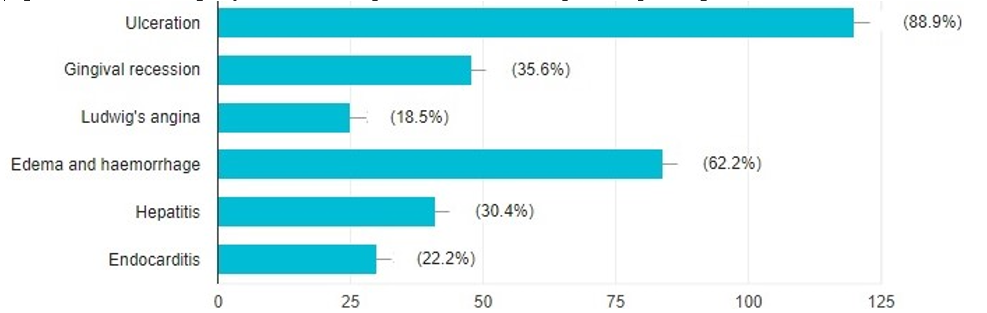
Figure 7
What according to you are the jewelry used for oral piercing?
78.1% were familiar with ring as an oral piercing jewellery 64.2% recognized stud as an oral piercing jewellery 13.9% identified barbell as jewellery and only 5% knew about labret.
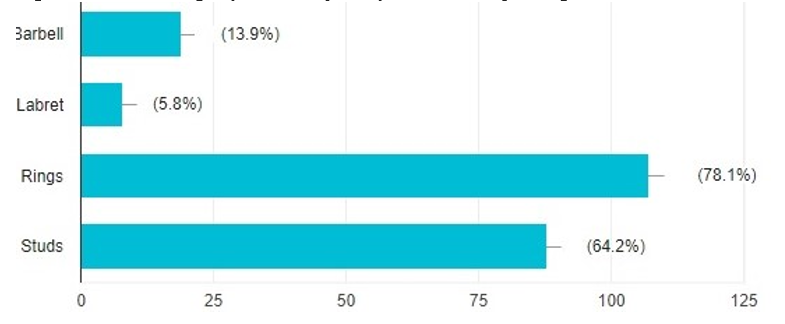
Figure 8
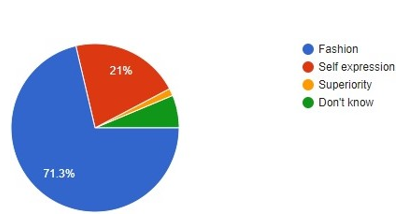
Why do you think people get their oral and perioral piercings done?
71.3% considered oral piercing as a fashion statement 21% believed it as a self-expression 1.4% regarded it as superiority and 6.3% didn’t know why people perform oral piercing.


Discussion
Oral and perioral piercing is just an ill wind that blows nobody any good. These piercings are performed in tattoo studios. Many of the piercers are not even licensed practitioners and thus piercing procedures are done without even giving appropriate anesthesia.7, 19 Some of them use the same needles to different person frequently without sterilization. Hence, various piercing failure cases have been reported worldwide. In fact, American Dental Association has put across an opposing statement against oral piercings.
“The American Academy of Pediatric Dentistry strongly opposes the practice of piercing intraoral and perioral tissues and use of jewellery on intraoral and perioral tissues due to the potential for pathological conditions and sequelae associated with these practices”.32
Ioannis et al, concluded that oral piercings results in harmful acute and chronic risk to both soft and hard tissues and they may eventually cause severe consequences.3 Cinzia et al., clearly explains how the oral hygiene practices changes after oral piercings.4 but in our study only 72% students knew about this fact and rest were unaware of the context. According to Hennequin-Hoenderdos et al., the rising popularity of body piercings in young adults, is determined by various factors, including the urge to fulfil social demands, establish a personal statement or enhance sexual appeal.33 Whereas in our study, 71.3% students considered oral piercing as a fashion statement. Moreover only 5.8% students in our study knew that labrets are also used as an ornament. Dermata. A et al., suggests that as a part of history taking questions related to piercings should be included.19 O'Dwyer JJ and Holmes A in their article, clearly describes how a carelessly placed labret caused trauma to lower gingiva causing gingival recession.28 In our study only 35.6% students’ marked gingival recession as a complication of oral piercing which obviously states how gingival recession is not considered as a serious complication.
Conclusion
Dentists are the paramount professionals in detecting such complications and hence they should be well aware and so requires comprehensive knowledge regarding sequelae of oral and perioral piercings. Dental students on the other hand are upcoming dentists who will treat the upcoming generation and thus play an important role in educating their peer groups and other patients. Although many dental students had a knowledge regarding harmful complications of oral and perioral piercing, but many pages are unturned with respect to its severity and how it affects the life of an individual after. Hence, students should encourage everyone to be aware of these ruinous procedures and discuss their detrimental effects with patients as much as they can. Students should also educate them about how the oral hygiene practices change after these jewellery, and how to properly maintain the oral hygiene. 33