Introduction
The advent of improved all-ceramic systems helps to achieve optimal esthetics and strength to withstand functional stresses. Also, the ability of these materials to bond to enamel and dentin has widened the applicability of metal free restorations.1, 2
Post and core as a foundation for the final restoration is often required for rehabilitation of endodontically treated and fractured teeth. The age old custom cast metal post and core used for restoration of non-vital anterior teeth results in unesthetic all ceramic crown restoration due to decreased translucency.3 Improvements in ceramic materials and porcelain bonding systems have paved way for successful metal-free restorations. Thus, utilising ceramic post and core has combined the advantages in terms of esthetic and mechanical properties. The case report presented describes rehabilitation of a patient with fractured anterior tooth using custom fabricated zirconia post and core along with full coverage all ceramic restoration thus providing optimal esthetics and durability.
Case Report
A 38-year-old female, teacher by profession reported to the Department of prosthodontics, with chief complaint of pain in upper right front region of jaw. Intraoral examination revealed grossly carious lesion wrt right maxillary canine with loss of the crown structure (Figure 1). Probing depths around the tooth were in physiological range and there was no pathological mobility. Radiographic examination confirmed pulpal exposure. Based on the clinical and radiographic findings, a diagnosis of Ellis class V fracture was arrived at. Based on the patient's esthetic requirements and biological considerations of preserving remaining coronal tooth structure and occlusion, a treatment plan was formulated to rehabilitate the patient with endodontics followed by custom made CAD/CAM fabricated all-ceramic post-core and full coverage restoration.
The treatment plan was devised to be completed in 3 phases.
Phase I - Endodontic treatment of the maxillary canine
Phase II- Prosthodontic management comprising of custom fabricated zirconia post and core along with full coverage all-ceramic restoration.
Phase III- Maintenance and follow up
The procedure was explained to the patient and an informed consent was obtained.
Clinical procedure
Phase I
Endodontic treatment was performed under rubber dam isolation and was completed in 2 appointments using gutta percha by vertical and lateral condensation method.
Phase II
Post space preparation- It was prepared using the 1.4 mm drill provided by the manufacturer. Five to six millimeters of gutta percha was maintained apically for adequate apical seal.
Post and core pattern fabrication- it was made with pattern resin and finished (Figure 2).
Tooth preparation- It was done following biomechanical principles with radial shoulder finish line. A 360° radial shoulder was prepared using a round end tapered fissure diamond (Figure 3).
(Shade matching- Shade matching for ceramic restoration was done (Vitapan Classical Shade Guide, VITA Zahnfabric, Bad Sackingen, Germany)
Laboratory Procedure
CAD-CAM milled Zirconia Post and core
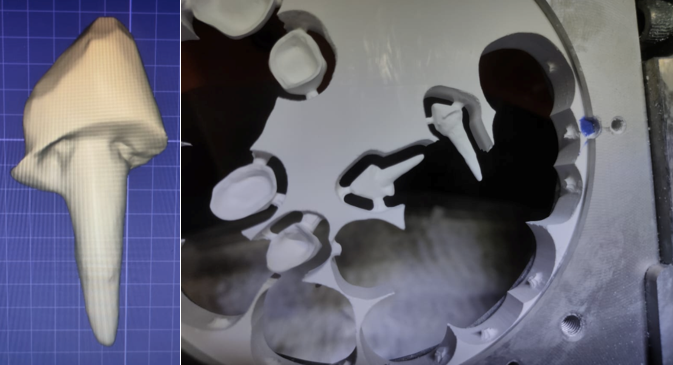
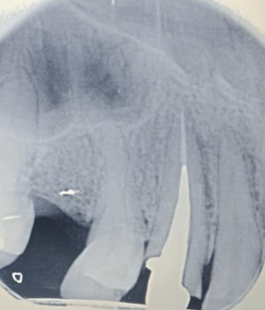
The pattern of the post was scanned using an optical scanner, milled in partially sintered zirconia block and sintered for eight hours and finishing done (Figure 4, Figure 5). Trial was done to verify the post adaptation and a radiograph was taken to confirm the same (Figure 6).
Post surface was air-abraded with 50-µm Al2O3 particles prior to cementation. It was luted with dual-cured resin cement (Medicept Self Cem) following the manufacturer’s instructions. After inserting the post into the canal, excess cement was removed, and polymerization was initiated using a polymerization lamp for 40 seconds (Figure 7).
Gingival retraction was done using a #00 retraction cord and a two step putty wash impression was made using a polyvinyl siloxane impression material (Aquasil Soft Putty/Regular Set Impression material, Dentsply DeTrey, Konstanz, Germany). Cast was poured in die stone.
CAD-CAM milled full coverage (Suprinity®) restoration
The prepared tooth was scanned using CAD-CAM technology (Ceramill Map 400+ scanner; Amann Girrbach AG). Designing of the crown was done on the scanned die using Ceramill Mind software with a provision of 50 μm space for cement film thickness. Margins were detected using automated function of the software. Designing was done to adapt the crown to prepared margin. Scanned data along with the designed coping of the crown was transferred to the milling unit and was milled out of Zirconia reinforced high strength glass ceramic, Suprinity® using Ceramill Rotomotion 2.5 mm burs. Restoration was carefully retrieved from the block, subjected to the crystallization process for 10 minutes and polished.
The restoration was evaluated for marginal fit shade, and occlusion prior to cementation, gingival retraction cord placed, and the restoration luted with a resin luting agent following the same procedure as during post cementation (Figure 8). Post rehabilitation, the biologic, functional and esthetic and the objectives were optimally achieved (Figure 9).







Discussion
Zirconia posts are gaining popularity as an ideal all-ceramic post as they provide optical properties for post/cores similar to that of all-ceramic crowns. 4 The German chemist Martin Heinrich Klaproth in 1789 discovered Zirconia as a metal oxide (ZrO 2). The stabilizers are added in pure zirconia for the fabrication of posts. Zirconium oxide is the strongest white-shaded ceramic in recent times. They are commonly known as yttrium-stabilized tetragonal zirconia polycrystals containing zirconium oxide (94.9%) and yttrium oxide (5.1%). This type of zirconium oxide is known for its high performance. When subjected to stress, the tetragonal crystal phase is transformed into monoclinic phase and an associated volumetric expansion (3-5%) takes place. This results in the development of internal stresses opposing the opening of a crack, thus increasing the resistance of the material to crack propagation. Therefore, stresses are absorbed and no crack formation occurs. Zirconium oxide has found profound applications in dentistry as it is the strongest and toughest ceramic available.5, 6
The advantage with the zirconia materials is its tooth-coloured shade, rendering the material compatible with all-ceramic crowns in the anterior region. In particular, a patient presenting with a high lip line and thin gingival tissue would need the use of a zirconia post with an all-ceramic crown to optimize the esthetic effect at the root, while maintaining an adequate strength. In addition, zirconia is indicated for teeth with severe coronal destruction, because composite materials lack the strength to resist deformation when used to support crowns.7, 8
This technique allows for a high level of adaptation to the remaining tooth structure. The ceramic core offers excellent dimensional stability, a strong bond between the post ceramic and core ceramic and forms an integral post and core structure, which acts as a monobloc.
However, the high rigidity of zirconia posts, can act as a predisposing factor for vertical root fractures. Hence, zirconia posts should not be used for patients with bruxism. Also, as it is difficult to grind away the zirconia posts, it becomes impossible for retreatment of the root canal treated teeth.9
The case presented in this report has been followed up over a period of 6 months and exhibited fracture, debonding, or change in esthetics.
Conclusion
In the case presented, zirconia post and core system resulted in high esthetic results and mechanical success. The advantage of this milled ceramic post was its strength and esthetics due to its one-piece construction. Hence, all-ceramic systems offer an exceptional esthetic alternative for anterior areas and can be considered viable treatment options to optimise esthetics and strength. Although a number of in-vitro studies are available in literature, clinical success judgement will require long term in vivo studies with a long follow up period to check the efficacy of zirconia to be used as endodontic posts thus opening gateways for further clinical research.