Introduction
Dentists employ vibrating hand-held tools during dental procedures, known as “hand pieces”. The vibration spectra of hand pieces used in dentistry contain high frequency components. Vibration is transmitted not only through the hand piece, but also through the work piece held by the dentist. The vibration emission of dental tools is dominated by high frequency components above 1000 Hz; 1, 2 the vibration from most industrial power tools is dominated by vibration at lower frequencies.3 It is well known that exposure to prolonged (i.e. for several years) exposure to vibration is harmful, and can cause various types of hand dysfunction. Most common are a loss of sensibility, blanching and decreases grip force in the hands that is, Hand-Arm Vibration Syndrome (HAVS). The symptoms of HAVS are characterized by neurological and vascular components. 4 There are concerns whether the frequency weighting within ISO 5349 reflects the risk of harm at high frequencies and the validity of the daily vibration exposure metric A(8), crucial to risk assessment, which inherently emphasizes vibration magnitude relative to exposure duration. 5 This study investigates the dose-response relationship derived using the exposure point system and ready reckoner based on a standardized questionnaire. It attempts to identify the most practicable exposure action and limit value measure that can be collected to aid in the health assessment of dentists exposed to hand-arm vibration.
Materials and Methods
Based on the study by S.H Bylund, 6 et al. assuming p=30% with 95% confidence interval and 10% allowable error (L) sample size estimated for the study was 84. Further assuming 10% non-response rate, the final sample size estimated for the study was 92.
The sample size was calculated using this formula, n=
Using a cross-sectional analysis, this study analyzed the incidence of hand-arm vibration on dentists and measured these results with a ready reckoner. The sample size consisted of 92 dentists in and around Mangalore, Karnataka, India. Data was collected using questionnaires and google forms.
The questionnaire was partly developed on the basis of earlier surveys.6 Questions were asked about years of working experience, often used vibrating hand-held tool i.e. aerotor or Piezoelectric scaler, duration of usage and the vibration magnitude of the vibrating tool. Questions concerning the neurological and vascular symptoms in fingers and hands, tremor and pain in the hand and neck were asked. To identify vascular symptoms, the dentists were asked ‘Do your fingers get white in cold?’ and ‘Do you have a sensation of cold in your fingers?’ To identify neurological symptoms, the dentists were asked about symptoms of numbness. 6 Questions concerning ergonomic load factors, joint related and neuromuscular related disorders were also included. Information was also collected on individual factors such as smoking or drinking habits, current work situation and other occurring occupational factors.6 The questionnaires were sent by google forms, e-mails and reminder letters were sent to the dentists who had not responded within 2 weeks. Reply forms where the dentists had marked ‘Hand-arm vibration are not the cause of my injury’ or ‘I don’t want to participate in this survey’ were not included in the study. The study was followed in accordance with the research ethics committee.
Descriptive statistics such as mean & standard deviation were used to represent quantitative data. Chi square test was used for the association of values of vibration magnitude with duration of usage and p<0.05 is considered as statistically significant. The prevalence was calculated on the percentage of the number of answers. The symptoms classified into ‘Yes/No’.
The dose-response relationship between vibration magnitude and exposure time was calculated with the ready reckoner.5 ‘Daily exposure’ means the quantity of mechanical vibration to which a worker is exposed during a working day, normalized to an 8-hour reference period.5
The calculation of daily exposure time of a dentist using vibrating hand-held tool was based on an 8-hour working day categorized into less than 1 hour and more than 1 hour. The vibrating hand-held tool often used during a dental procedure are aerotor and a piezoelectric scaler which ranges from 20kHz-45kHz (frequency). Categorized into 2 groups: 20-35kHz and 36-45kHz. The frequency of these dental tools was converted into rpm unit i.e. frequency multiplied into 60 and then calculated into acceleration (m/s) using an online convertor. The following exposure time (T) was taken as 1 hour to 3hours. Therefore, calculated the 8-hour energy-equivalent vibration, aeq(8) = √T/8.aT where aeq(8) is the 8-hour equivalent acceleration. T the actual exposure time in hours and aT acceleration (m/s) during the period T hours.3
The vibration magnitude was categorized into the following 2 classes: 7m/s2 - 22m/s2 and 13m/s2 - 28m/s2. The total daily exposure to vibration is a function of both the magnitude and the duration of vibration. This is expressed in terms of the frequency-weighted eight hour energy equivalent level and reported in m/s² A(8).4 The ready reckoner or exposure points is easier to work with than A (8) values: exposure point’s change simply with time: twice the exposure time, twice the number of points. For Hand-arm vibration- a) The daily exposure limit value (ELV) is 5m/s2 A (8) is equal to 100 points. b) The daily exposure action value (EAV) is 2.5m/s2 A (8) is equal to 400 points.5
The daily exposure limit value (ELV) is the maximum amount of vibration an employee may be exposed to on any single day. The daily exposure action value (EAV) is the level of daily exposure to vibration above which we are required to take certain actions to reduce exposure. In the ready reckoner, the values contain a specific color which tells whether the exposure exceeds, or is likely to exceed, the action value or limit value.5
Results
The study group comprised of 92 dentists. The profile obtained from age wise distribution of respondents were 76% more than or equal to 35 years of age. Gender wise distribution was obtained as 56.5 % of females compared to males and 85% of the dentists had more than or equal to 10 years of experience. The daily exposure time showed 79% of the dentist’s work for more than 1hour and aerotor was the most common vibrating hand-held tool used by 74% of the dentists. (Figure 1, Figure 2)
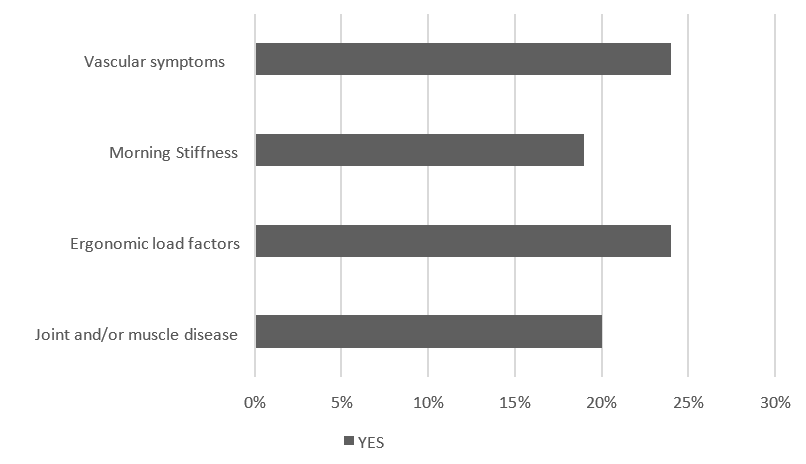
Numbness, pain, tremors and tingling sensation were the most common symptoms observed.
Morning stiffness and symptoms from the ergonomic load factors were also frequent complaints. 24% of dentists reported pain/numbness/tremors/tingling sensation in their fingers & symptoms due to ergonomic load factors. 19% of dentists had experienced morning stiffness in their dominant to non-dominant hand. 20% of the dentists showed suffering from muscle and/or joint diseases, principally torticollis, arthritis and back pain. 9% of the dentist’s experienced fingers getting white in cold and 10% of them suffer from some kind of hearing loss. These responses were not related to smoking or alcohol consumptions. The current prevalence of all symptoms except vascular symptoms was significantly higher among the dentists. These responses exposed to high levels of hand transmitted drills raises the possibility that dentists may be at risk of hand-arm vibration syndrome. (Figure 3)
The magnitude of vibration transmission per day among the dentists differed between the two categories. 40 out of 92 dentists preferred working with tools ranging between 7-22m/s2 and 52 out of 92 used vibrating tools between 13-28m/s2 i.e. 55% of the dentists worked above the exposure limit value (Table 1). In determining the association of the vibration magnitude with duration of usage did not show a significant difference. 59 % of the dentists worked for more than 1 hour in relation to 13-28m/s2 (Table 2, p>0.05).
The middle-aged dentists with more than or equal to 10 years of working experience are being exposed to more than 5m/s2 of vibration magnitude. Average vibration magnitude values were calculated over the course of 8-hour work day using ready reckoner. Therefore, 85% of the dentists are likely to be at or above exposure limit value.(Figure 4)
Table 1
Determining the magnitude of vibration transmission per day among the dentists.
|
Magnitude of the vibrating tool |
Number of dentists n=92 |
Percentage |
|
7 m/s2 - 22 m/s2 |
40 |
45% |
|
13 m/s2 - 28 m/s2 |
52 |
55% |

Discussion
This study presents prevalence data on exposure point system and ready reckoner among dentists exposed to hand-arm vibration. The prevalence data showed 85% of the dentists at/above exposure limit value. Exposure limit value (ELV) was observed to be more among dentists with more than or equal to 10 years of working experience. The relative risk of getting a vibration injury is high and immediate action is required to reduce exposure with duration of usage. The ready reckoner consists of exposure points which change simply with time i.e., twice the exposure time, twice the number of points. Exposure duration is only the trigger time during which the hands are actually exposed to vibration. The exposure limit value is equal to 400 points.5 Minimization of risk will involve controlling vibration exposures but also other confounding factors such as ensuring tools are ergonomically designed and that working postures are optimized.4 This serves as a good guide to evaluate the hand-arm vibration exposure and also offers suggestions w.r.t reducing associated risks.5
A study found that using simple years of exposure was a weak predictor of HAVS or its increasing severity. The calculation of cumulative hours across all vibrating tools used was a more powerful predictor.7 Our study involved the years of vibration, total hours of use and magnitude vibration. But no study was conducted regarding the ready reckoner and were also biased.
Although the prevalence of such disorders has been reported as relatively low among dentists,8 exposure to vibration from dental tools has been associated with early stages of hand-arm vibration syndrome for several years. 9, 10, 11 More recently, Bylund et al.6 showed that, in Sweden, the relative risk of developing HAVS was more significant for these dental professionals than for populations of female industrial workers such as for users of grinders and impact tools. The cause-effect relation between vibration and chronic disorders has been opaquer: the elapse of time between cause and effect and the complexity of both the cause and the effect have helped to conceal their relation. Knowing that vibration causes injury leads to attempts to represent the vibration by means of numbers (measurement). Vibration can be measured without knowledge of the effects it produces. 3 To discern the relative or absolute severity of the vibration (evaluation), or to identify the likely consequences of exposure to the vibration (assessment), it is necessary to have knowledge of the cause-effect relation between vibration and injury.3
In this study, we found that dentists are relatively at risk. The hand-arm vibration symptoms could be caused by ergonomic or non-environmental factors but there is also a possibility that dentists are vulnerable to vibration. Although the magnitudes of vibration will not approach the exposure action value or exposure limit value as set out in the directive, risks will still need to be minimized. This could be achieved by reducing exposure times, health surveillance, use of improved handpieces and other equipment, and by improving the overall ergonomics of the workplace. This study helps to move on from the gaps and get closer to those refined results for future references.
Conclusion
This study definitely answers the questions regarding the exposure to hand-arm vibration on dentists. This can result in a condition known as Hand-arm vibration syndrome (HAVS) that includes vascular and neurological components. It is most often seen amongst those industrial power tools, but there is evidence that dentists are also at risk. Further studies are needed to establish casual relationships and develop preventive measures.