Introduction
Discovery of foreign objects in root canal is uncommon and rare. Ingestion or aspiration of the foreign object could be scaring and difficult situation. Impaction of foreign objects in pulp chamber is commonly seen in kids who have practice of placing different objects in oral cavity. Various foreign objects deposited in the pulp chamber of tooth have been reported such as paper clip, stapler pins, pencil lead, needles, dressing pin etc. Because of inability for complete removal of infection present in canal, foreign objects may become sources of infection in future. Thus these objects need to be removed for complete disinfection in the root canal.1, 2, 3, 4, 5 This case report describes a clinical case in which a sewing needle was inserted into the root canal by the patient and thus attempt was done for its retrieval and followed by restoring the tooth with template technique using direct resin restoration.
Case Report
A 14-year-old male patient reported with his gaurdian to the Department of Conservative Dentistry and Endodontics, with a chief complaint of broken tooth in upper left front tooth region due to trauma and wants the treatment of same. Patient's history and intra-oral examination exhibited following findings: History of trauma to maxillary anterior teeth; 3 years ago. Fractured tooth 21 has Ellis class III fracture with discoloured crown. The same tooth also showed a small incisal opening into the pulp chamber and there was no pain associated with it.
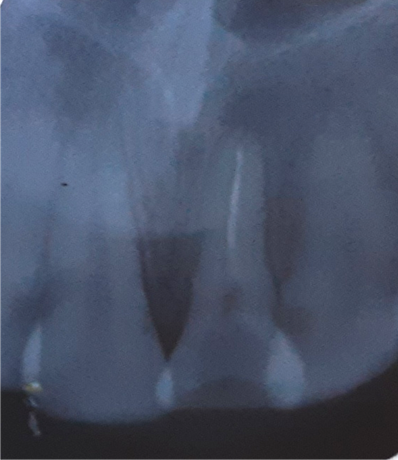
Endo-Ice (Coltene) was used with cotton pellets to test the response of nerve fibres on the middle third of the tooth and 21 showed no response and a normal response exhibited in teeth nos. 11, 12 and 22. Intra-oral periapical radiograph of tooth 21 showed, the presence of slender, radiopaque object. After taking the patient into confidence a careful enquiry of patient revealed that, the patient frequently used sewing needle as a tooth pick to clean the lodged food from the same tooth. After evaluating the clinical and radiographic findings; the following treatment plan was advised
To retrieve foreign object by a simple non-surgical technique.
Endodontic treatment of tooth 21 followed by direct composite restoration by direct composite using template technique.
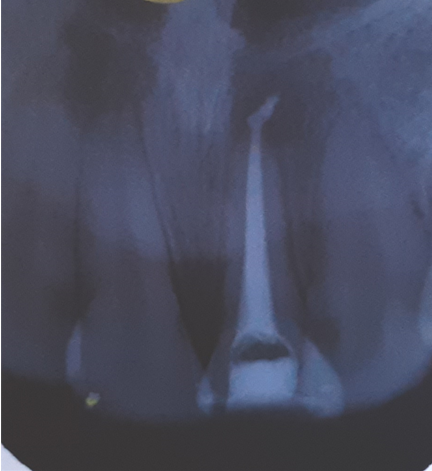
The tooth was isolated with a rubber dam and the access was modified. Attempts to bypass the metallic object were done and with the help of braided technique, it was retrieved. After loosening and removing most of the metallic objects using the H file, the rest of the object was retrieved by irrigation, using 5.25% sodium hypochlorite (NaOCl).
The working length was determined with an electronic apex locator (Canal Pro Coltene). Canal was prepared with the NeoEndo Rotray system (Orikam) under copious irrigation with 5.25% NaOCI. Then root canal was dried with sterile paper points, dressed with calcium hydroxide (ApexCal) and restored with a temporary filling (Cavit G). On the second appointment after one week, temporary filling was removed and the root canal was irrigated with 5.25% NaOCI and 17% EDTA. For the final irrigation, 5.25% NaOCI was used. The canals were dried with sterile paper points and obturated by the cold lateral compaction technique with Sealapex and gutta-percha. The tooth was restored with a light-cured composite resin by use of template technique.
The unsupported enamel was removed via 45 degree bevel. Preliminary impressions of both the arches were made and study models were made in dental stone and mock preparation of the lost tooth structure with modeling wax was done. After crown build up, the cast was duplicated by using template of putty impression material. Labial surface of the putty template was removed up to middle third of the crown, to aid in the reconstruction of the lost tooth structure. A clinical try-in of the template was done to ensure adequate fit. After appropriate shade selection of the composite material, the build-up was done to restore the fractured teeth quickly with minimal post-restoration finishing.







Discussion
If the root canal is open, the patient may try to clean the obstructing food substances from the canal with various objects that may break and get lodged in the pulp space. Foreign objects in the root canal can be a source of infection and should be removed. This may sometimes be very difficult because of the shape, size and position of the foreign body. The degree of difficulty depends also on the time that has elapsed since the foreign body was inserted in to the root canal. The removal of foreign objects is sometimes difficult and the success rate has been reported to be 55% to 79%.
Many methods are described for removing broken instruments or objects within root canals, such as hand instrumentation, braided technique, ultrasonic devices, the Masserann Kit, the Canal Finder System or surgical methods. If much time has elapsed with a metallic foreign body in the root canal there is the possibility of corrosion as in this case. Corroding metallic bodies can become more fragile and, as in this case, may break when retrieval is attempted. Foreign bodies in the root canal system should be removed for successful endodontic treatment as these objects can clearly cause infection and pain. Non-surgical endodontic treatment should be tried first, but in some cases endodontic surgery may be required. Management of patient’s with anterior tooth fracture provides great challenge to the clinicians both from a functional and an esthetic perceptive. Treatment objectives may vary depending on the age, socio-economic status of the patient and intraoral status at the time of treatment planning. Greater risk of biological and mechanical failure due to extensive tooth preparation occurs in fixed prosthesis, thus direct composite build up was selected as treatment of tooth as the patient was young.
Conclusion
Removal of foreign objects from root canals has been widely discussed and various techniques have been suggested. Foreign bodies in the root canal system if present should be removed for successful endodontic treatment as these objects can clearly cause infection and pain. With appropriate diagnostic and treatment tools, as well as good patient cooperation, management of foreign object removal from root canals can be quite straightforward. Non-surgical endodontic treatment should be tried first, but in some cases endodontic surgery may be required.