Introduction
The principle explanation behind the disappointment of endodontic treatment success rate is deficient information about the anatomical variety of root canals. A canal is frequently left untreated in light of the fact that the dental specialist neglects to perceive its quality either because of lack of information on root canal morphology or because of absence of experience and proficiency. The dentist must have a thorough information on root canal morphology before beginning endodontic treatment. For good prognosis following root canal treatment, the whole canal system framework must be thoroughly introspected, debrided, and filled. In this manner, clinicians must be acquainted with the different root canal designs. 1, 2
Different studies have been conducted on root canal morphology of extracted mandibular incisors and have revealed a preva-lence of two canals in 12–35% of the cases. The prevalence of numerous canals in all single mandibular incisors of the same patients has not been accounted for. 2
This case report presents a rare case report with 2 canals in the lower anteriors with periapical radioluceny indicated for endodontic treatment, each having two separate canals which unite in apical third. 1, 3, 4
Case Description
A 38-year-old man reported to the Department of Conservative Dentistry and Endodontics of Modern Dental College & Research Centre, Indore with chief complaint of pain & swelling in lower anterior teeth, moderate, dull aching, and intermittent pain in the lower right front region of the teeth for 2 months. On clinical examination, 31, 32, 41, and 42 were tender on percussion. The patient's medical history was non-contributory. The teeth were not mobile and periodontal probing around the teeth was within physiological limits.
A diagnostic radiograph revealed a coronal occlusal caries involving enamel and dentin, a coronal disto occlusal radiolucency involving the pulp space and widening of the periodontal ligament space with severe attrition in all lower incisors. The radiographic examination showed the presence of two separate canals at the coronal and middle one-third of root and merging at the apical third of the root, periapical radioluceny assosiated with 31, 41 is indicative of periradicular spread of pulpal infection. Based on the clinical and radiographic findings, diagnosis of symptomatic apical periodontitis was considered.
Local anesthesia was administered and caries was removed from the carious teeth. Conventional access cavity preparation was done with Endo Access Round Diamond Bur (Dentsply/Maillefer, Ballaigues, Switzerland). Lingual modification of conventional access cavities was done to locate extra canal lingual to the main canal. Patency filing with 10 k file and negotiation of two root canals were done with a size 15 K-file in lingual canal and size 20 K-file in buccal canal. Radiographic working length measurement was done with Kodak. RVG 5100 Digital Dental Unit (Kodak) and confirmed using apex locator (Root ZX J Morita). Cleaning and shaping of root canals were done using K-files (Dentsply, Maillefer) by conventional method till 30 K-file.
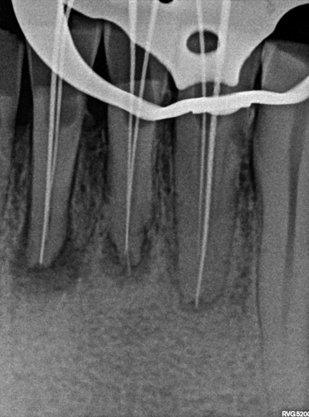
Radiographic examination revealed presence of 2 canals with 31, 32, 41, and 42. Two root canals were observed in all lower incisors (Figure 1).
A possibility of two canals was suspected and the treatment for 31, 32, 41, and 42 was planned accordingly.
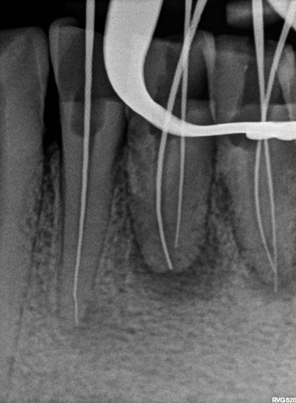
The access openings of all mandibular incisors was enlarged buccolingually and extended into cingulum gingivally. This revealed the presence of a lingual canal. The patency was checked using a no. 10k file. Working length was determined by placing a 20 no. K file in the buccal canal & 15 no. K file in the lingual canal using digital radiography (Figure 1, Figure 2 ). The presence of extra canals were confirmed using different angulations while taking radiographs. Biomechanical preparation was carried out using conventional hand instruments. 3% of sodium hypochlorite and 17% EDTA were used for irrigation. The canals were rinsed with normal saline and recapitulated after each instrument progression.
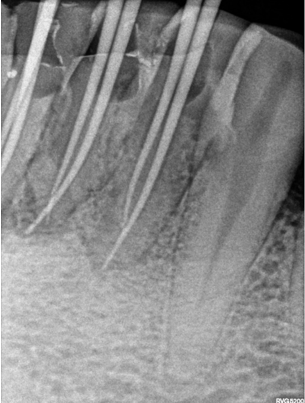
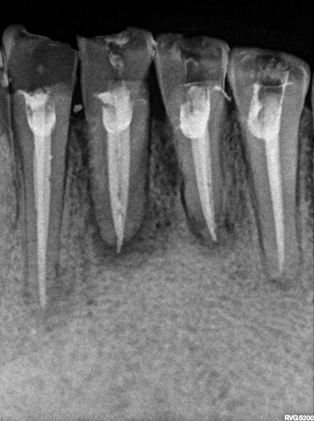
During the next visit after four days; all teeth were asymptomatic and obturation was done using single cone obturation technique. Radiographs were taken at different angulations (20 degree right and 30 degree left horizontal beam angulation) for visualizing master cones of two canals (figure 3).5 Canals were obturated with single cone technique using sealer sealapex (zinc oxide based root canal sealer). Access cavity were restored with glass ionomer cement (figure 4).
Discussion
In highly complex root canal morphologies, it is a challenge to find adequate access and perform biomechanical preparations. Mandibular incisors due to their small size and internal anatomy could also be most difficult access cavities to organize. Complete removal of the lingual shoulder is critical, because these teeth often have two canals that are buccolingually oriented and the lingual canal most frequently is missed. In order to avoid missing this canal, the dentist should extend the access preparation towards the cingulum. When there are two canals, the buccal canal is generally easier to locate and is usually straighter.
The lingual canal, which is usually shielded by lingual shelf.6 as encountered in this case, extension of the access opening lingually beneath the cingulum revealed the missed lingual canals in mandibular incisors.
For a general practitioner, it is very difficult to locate a second lingual canal, since it’s expectancy is low.
The most common reason for endodontic treatment failure in mandibular incisor teeth is due to failure in locating, debriding, and obturating the missed lingual canal. Prior to starting endodontic treatment, a thorough radiographic evaluation is necessary.
Modification in access opening and initial buccolingual widening of mandibular incisors and gingival extension beneath the cingulum must be thoroughly introspected for a possible second canal lingually. Magnification is very useful in visual inspection under dental operating microscope or dental loupes.
Conclusion
The most common reason for failure of endodontic treatment of mandibular incisor can be due to the inability to detect and treat second root canal, most often lingual canal. Thus, careful interpretation of radiographs taken from different angulations is must. Practice of modification of access cavity buccolingually and gingivally beneath cingulum and visualizing access preparation under dental operating microscope or dental loupes, will help to detect additional lingual canal if present in each mandibular incisor. 7