- Visibility 1.6k Views
- Downloads 102 Downloads
- Permissions
- DOI 10.18231/j.idjsr.2024.003
-
CrossMark

Abstract
Occlusal splints are described as “Any removable artificial occlusal surface affecting the relationship of the mandible to the maxilla used for diagnosis or therapy. Prosthodontic management of Temporomandibular joint disorders (TMDs) has been a controversial topic. The purpose of this article is to make prosthodontists aware about use and significance of splints in dealing with temporomandibular disorders (TMDs) the by usage of easy and less difficult remedy.
Introduction
Occlusal splint therapy is defined as “the art and science of establishing neuromuscular harmony in the masticatory system by creating a mechanical disadvantage for parafunctional forces with removable appliances”. [1] Occlusal splint is a relaxing and diagnostic, reversible device.
According to the (GPT) Glossary of Prosthodontic Terms [8th ed.], “occlusal splint is defined as any removable artificial occlusal surface used for diagnosis or therapy affecting the relationship of the mandible to the maxilla.
It may be used for occlusal stabilization, for treatment of temporomandibular disorders, or to prevent wear of the dentition.”
A bite splint is a valuable diagnostic tool in carefully selected cases if made properly with adjustment. A well prepared and fabricated occlusal splint helps in maintaining harmonious relation with masticatory muscles, joints, bones, ligaments, disc assemblies. It offers a notably easy, much less high priced and much less dangerous approaches to make reversible modifications withinside the occlusion. Occlusal splint remedy is useful in diagnosis and remedy of diverse temporomandibular disorders. [2]
The major purpose of Occlusal splint remedy is to the Temporomandibular joint discs from the dysfunctional forces, which can also additionally cause trauma to the joint and everlasting displacements. Others functions are to enhance muscle features and to alleviate any ache associated with TMJ. [3], [4], [5], [6], [7], [8], [9], [10]
Occlusal splint therapy for recommended for the following functions:
Occlusal splint remedy is encouraged for the subsequent features:
To keep away from damage to oral tissues in individuals with parafunctional conduct.
To stabilize un-stable occlusion
To relieve jaw muscle ache in sufferers with temporomandibular disorders (TMDs) and pressure associated ache of muscular origin.
To get rid of the results of occlusal interferences.
How do Splints Work?
Following few concepts explain how the occlusal splints work.
Avoiding the contact in (MIP) maximum intercuspation
Occlusal splints help mandible to close mandible in new posture thereby resulting in a new muscular balance. This will protect the TMJ and teeth by avoiding clenching of teeth.
Force distribution
The forces generated in parafunctional habits such as bruxism are much higher than the normal masticatory forces which are distributed by occlusal splints across the masticatory system.
Normalizing the proprioception via periodontal ligament (PDL)
Various proprioceptive fibers of periodontal ligament send signals to central nervous system (CNS), thereby triggering the muscle styles with a purpose to defend them from overload. Occlusal splints deplete the forces performing on individual tooth through covering a bigger surface area. A hyperactive muscle which is fatigued for long term can display signs and symptoms of ache. If hyperactivity is discontinued the ache will typically relive.
Guiding condyles to seat in (CR) centric relation position
Ideally condyles should rest in anterosuperior position where the superior belly of lateral pterygoid muscle obtains the full extension. When lateral pterygoid undergoes hyperactivity, the disc is pulled antero-medially to origin of muscle which results in displacement. A well fabricated splint results in a proper occlusion with relaxation of elevator and positioning muscles, allowing the articular disc to obtain its anterosuperior position over condyle head. Occlusal splints can be adjusted with a vertical dimension height which exceeds the physiologic interocclusal distance. [11], [12], [13], [14]
Cognitive awareness theory
This theory states that the presence of any foreign object in mouth would likely change the tactile stimulation, decrease in oral volume and making patient more conscious about its position. Here that purpose is served by occlusal splint. As cognitive awareness is increased, the factors contributing to this disorder are decreased.
Types of Occlusal Splints
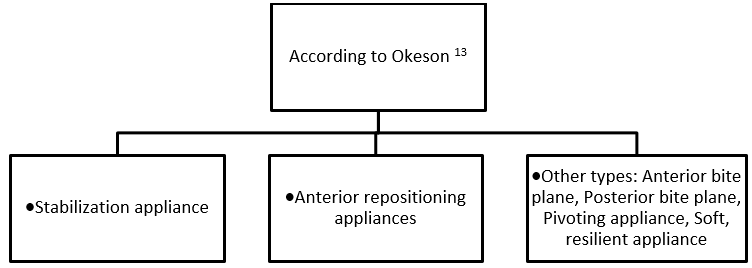
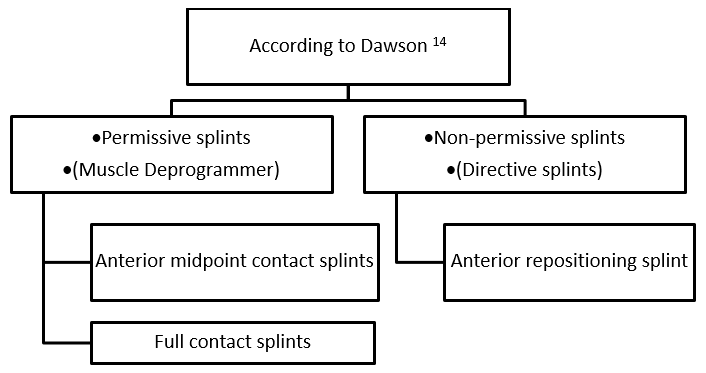
Permissive splints
Permissive splints are used to free up the occlusion to eliminate deviating teeth inclines from contact. This removes the etiology and impact of muscle in co-ordination. The condyles are then allowed to go back to their accurate seated position in centric relation if the situation of the articular components permits. Permissive splints also are known as as muscle deprogrammers.
The forms of permissive splints are anterior midpoint contact splints and complete contact splints.
Directive splints
These are used while the condyles had to be positioned in a particular function. The most important purpose of this splint is to place or align the condyle-disc relationship properly. Directive splints are designed to place the mandible in a particular relationship to the maxilla.
Specific Uses of Different Types of Splints
Stabilization splint
Stabilization splint is also recognized by the name the Tanner appliance, the advanced repositioning splint, the Fox appliance, the Michigan splint, or the centric relation appliance.([Figure 3])
The stabilization splint is made from hard acrylic splint which gives a transient and removable perfect occlusion. Stabilization splint gives an ideal occlusion thereby lowering abnormal muscle activity and generating neuromuscular balance.[15], [16] It need to be worn best at night. The affected person needs to be kept on follow-up at normal intervals. After a duration of successful splint therapy (2 to three months), sufferers may be weaned off the splint. A stabilization splint gives centric relation (CR) occlusion, removing posterior interference, providing anterior guidance and offers stable occlusal relationships with uniform tooth contacts all through the dental arch.

Indications
Muscle hyperactivity
Myospasms or myositis
Parafunctional activity
Masticatory myalgia and TMJ arthralgia
Anterior repositioning splint
The anterior repositioning splint guides the mandible in a function i.e., anterior position to the centric occlusion which allows the condyle in attaining extra favorable position in glenoid fossa. This position is ahead to the most intercuspation position (MIP) of the patient and influences the physiological-topographical relationship of the disc condyle complex.19, 20 The anterior repositioning splint locates a patient`s mandible and TMJ into an anterior position that allows you to decrease a TMJ click that is going on throughout an opening and closing of the jaw. The anterior repositioning splint is commonly positioned at the maxillary arch with an anterior ramp which first engages mandibular tooth on preliminary closure and shifts the jaw ahead into final closure, whilst all mandibular tooth is in contact with the splint. This position gives an extra favorable condylo-discal relationship within the fossa in order to maintain normal function. This removes the signs and symptoms of condyle disc interface disorder.([Figure 4] )
Indications
Disc derangement disorders
Intermittent jaw locking with limited range of motion
Joint sounds
Persistent TMJ arthralgia
Intermittent or chronic locking of the joint Inflammatory disorders (e.g. retrodiscitis)
Disc-interference disorders

Anterior bite plane
The anterior bite plane is a hard acrylic appliance worn over the maxillary teeth and provides contact with only the mandibular anterior teeth. The purpose of anterior bite plane is to disengage the posterior teeth and thus eliminating their influence in the function and dysfunction of the masticatory system.([Figure 5])
Types of anterior bite plane: Anterior jig, Hawley with bite plane, Lucia jig, Sved plate21, anterior deprogrammer.

Indications
Muscular disorders related to orthopedic instability or an acute change in the occlusal condition
Parafunctional habits related to unfavorable posterior tooth contacts
Acute disturbance in occlusion
Bruxism
Posterior bite plane
The posterior bite plane is usually fabricated to cover the mandibular teeth and made up of hard acrylic located over the posterior teeth and connected by a cast metal lingual bar. The main purpose of the posterior bite plane is to achieve major alterations in vertical dimension and mandibular repositioning. The Gelb splint 22 is a type of posterior bite plane.([Figure 6])
Indications
Severe loss of vertical dimension.
When major changes in anterior positioning of the mandible are required.

Pivoting splint
It is a hard acrylic appliance that covers one arch and usually provides a single posterior contact in each quadrant. This contact in this splint is usually established as far posteriorly as possible. ([Figure 7])
Indications
For the treatment of symptoms related to degenerative joint diseases.
Anterior disc displacement without reduction of TMJ
To unload the articular surface of the joint caused by decrease in inter-articular pressure
To reduce interarticular pressure and thus unload the articular surfaces of the joint.
Treating joint sounds.

Soft or resilient splint
The soft splint is an appliance made from resilient material and usually adapted on the maxillary teeth. The main purpose is to achieve even and simultaneous contact with the opposing teeth. It is quick to fabricate and can be provided in case of emergency treatment for a patient who presents with an acute TMD.([Figure 8])
Indications
Bruxism and clenching.
Prevention of trauma during sports (athletic splint).
Reducing symptoms of temporomandibular disorders (joint dysfunction and myalgia.

Bite splint
Bite splint doesn’t extend on facial or buccal surfaces of teeth but it covers the palatal area. It is usually used in patients who use splint for esthetic purpose in daytime as it is not visible.([Figure 9])

Cap splint
A cap splint can be used as an intermediate between a splint and a fixed bridge. It is useful for fabrication of temporary reconstruction. The occlusal surface is of acrylic and rest part is in metal.([Figure 10])

Splints for protection of oral tissues
The most common reason for fabrication of an occlusal splint is to protect the teeth from excessive abrasion in bruxism patient, several designs of splints are designed to protect cheeks and tongue in patients with oral parafunctional habits (such as bruxism, cheek biting and tongue thrust). These patients may have relief from a splint with extensions or enlargements designed in such a way that it keeps the cheeks from being pinched or the tongue from pressing against the lingual surfaces of the teeth.
Combination splints
Artificial teeth can be added to splint to replace the missing teeth. A Shore splint is an example of such splint which can function as a temporary partial denture by adding artificial teeth to it. There are various combinations of occlusal splint and orthodontic appliances. A removable bionator appliance is one such appliance that can act both as an orthodontic and as a repositioning appliance. An “invisible retainer” can simultaneously act as a soft acrylic splint.
Conclusion
Occlusal splint therapy has been used for many years in the diagnosis and treatment of various temporomandibular disorders. If TMDs left untreated it can lead to worsening of its symptoms which can extend beyond the jaws. Variety of designs are described in the literature. There are different types of splints that are used to treat different conditions. A thorough examination and differential diagnosis is necessary to know the decision regarding the appropriate role of splint therapy for each problem. The goal of this article was to make dentists aware of importance of splints in managing temporomandibular disorders (TMDs) using simple therapy.
Source of Funding
None.
Conflict of Interest
None.
References
- Dylina T. A common-sense approach to splint therapu. J Prosth Dent. 2001;86(5):539-45. [Google Scholar]
- Kreiner M, Betancor E, Clark GT. Occlusal stabilization appliances. Evidence of their efficacy. J Am Dent Assoc. 2001;132(6):770-7. [Google Scholar]
- Ash M. Current concepts in the aetiology, diagnosis and treatment of TMJ and muscle dysfunction. J Oral Rehabil. 1986;13(1):1-20. [Google Scholar]
- Nelson S. Principles of stabilization of bite splint theory. Dent Clin North Am. 1995;39(2):403-21. [Google Scholar]
- Attanasio R. Intraoral orthotic therapy. Dent Clin North Am. 1997;41(2):309-24. [Google Scholar]
- Boero R. The physiology of splint therapy: a literature review. Angle Orthodontist. 1989;59(3):165-80. [Google Scholar]
- Re J, Perez C, Darmouni L, Carlier J, Orthlieb J. The occlusal splint therapy. J Stomat Occ Med. 2009;2:82-6. [Google Scholar] [Crossref]
- Gibbs C, Mahan P, Lundeen H, Walsh E. Limits of human bite strength. J Prosthet Dent. 1986;56(2):226-9. [Google Scholar]
- KHolmgren, Sheikholeslam A, Ruse C. Effect of full arch maxillary occlusal splint on parafunctional activity during sleep in patients with nocturnal bruxism and signs and symptoms of craniomandibular disorders. J Prosthet Dent. 1993;69(3):293-7. [Google Scholar]
- Williamson E, Lundquist D. Anterior guidance and its effect on electromyographic activity of the temporal and masseter muscles. J Prosthet Dent. 1983;49(6):816-23. [Google Scholar]
- Manns A, Miralles R, Santander H, Valdivia J. Influence of vertical dimension in the treatment of myofascial pain dysfunction syndrome. J Prosthet Dent. 1983;50(5):700-9. [Google Scholar]
- Manns A, Miralles R, Cumsille F. Influence of vertical dimension on masseter muscle electromyographic activity in patients with mandibular dysfunction. J Prosthet Dent. 1985;53:243-7. [Google Scholar]
- Okeson J. . Management of temporomandibular disorders and occlusion. 1998. [Google Scholar]
- Dawson P. . Evaluation, diagnosis and treatment of occlusal problems. 1989. [Google Scholar]
- Gray R, Davies S. Occlusal splints and temporomandibular disorders: why, when, how?. Dent Update. 2001;28(4):194-9. [Google Scholar]
- Kurita H, Kurashina K, Kotani A. Clinical splint of full coverage occlusal splint therapy for specific temporomandibular disorder conditions and symptoms. J Prosthet Dent. 1997;78(5):506-10. [Google Scholar]
- Abstract
- Introduction
- How do Splints Work?
- Avoiding the contact in (MIP) maximum intercuspation
- Force distribution
- Normalizing the proprioception via periodontal ligament (PDL)
- Guiding condyles to seat in (CR) centric relation position
- Cognitive awareness theory
- Types of Occlusal Splints
- Specific Uses of Different Types of Splints
- Stabilization splint
- Anterior repositioning splint
- Anterior bite plane
- Posterior bite plane
- Pivoting splint
- Soft or resilient splint
- Bite splint
- Cap splint
- Splints for protection of oral tissues
- Combination splints
- Conclusion
- Source of Funding
- Conflict of Interest
- References